School-Based Mental Health Initiatives Challenges and Considerations for Policymakers

Photo: Stephen Welstead / Stone via Getty Images
Executive Summary
School-based mental health initiatives have expanded over the past half-century. In recent years, troubling increases in the prevalence of school violence and youth emotional distress have prompted a sense of urgency among policymakers, leading to the bipartisan action of committing billions of dollars annually in federal funding to bolster these programs.
But school-based mental health initiatives face fundamental challenges that warrant more thoughtful attention: mental health interventions for youth are not a panacea and warrant judicious utilization; the goals of the education and mental health systems are often in conflict; and vague policy, guidance, and expected outcomes undermine accountability and confuse responsibilities within and across systems.
Policymakers and education authorities should be clear-eyed about these challenges and the unintended consequences of administering mental health services through the education system. A decades-long track record of inconsistent marginal benefit, poor implementation, and some evidence of harm tempers confidence that effective, comprehensive school-based mental health services are attainable or desirable.
Key Findings
- There is a lack of high-quality evidence to support school-based mental health initiatives. Rigorous evaluations of universal programs on mental health literacy, awareness, prevention, and screening—and of many social-emotional learning programs—find neither reduced rates of mental health conditions nor improved academic outcomes.
- The concept of school-based mental health, as currently delivered in typical neighborhood public schools, is incoherent because it primarily serves youth who are not specifically in need of mental health treatment, while insufficiently serving those with mental disorders.
- While some youth can benefit from high-quality mental health services, universal mental health programs carry underestimated potential harms: directly, through poor-quality care, overdiagnosis, and misallocated spending; and indirectly, through wasted class time and reduced accountability in the mental health and education systems.
- Federal agencies responsible for school-based mental health programs provide no meaningful or coordinated guidance on essential questions such as what it means for a program to be effective, what expectations exist in “mental health deserts,” and how schools should sort through numerous overlapping initiatives.
Federal policy should make clear that the core goal of the public education system is to provide academic learning in preparation for productive participation in society, while the core responsibility of the public mental health system is to address untreated serious mental illnesses and serious emotional disturbances in youth. Neither system is obligated to carry out these goals through the approach of trying to improve mental health and wellness of everyone in society. That approach, in fact, has been counterproductive and has reduced accountability in both systems.
Universal mental health and wellness programming should be rolled back, and schools should instead pursue structural solutions such as setting and following school-wide behavioral expectations and maintaining full in-person school days. Youth mental health policy should prioritize serving youth with current cases of mental disorders across a full continuum of care.
Introduction
What Is School-Based Mental Health?
The focus of this report is on interventions delivered in K–12 neighborhood public schools.[1] A vast array of commercially available programs, conceptual frameworks, and approaches to school-based mental health are not unanimously recommended, applied, or agreed upon.[2] This poses a challenge to any comprehensive description or evaluation of school-based mental health.[3]
These programs are often categorized in a tiered structure, depending on how targeted they are and on the extent to which they are geared toward either prevention or treatment of mental illness. Table 1 describes how programs and services might fit into this prevention-oriented structure.
In Tier 1 are universal prevention programs, which are administered to all students, regardless of suspected or demonstrated need for mental health treatment. Tier 2 consists of more targeted prevention programs, aimed toward students considered at risk of developing mental illness, usually based on adverse environmental or familial characteristics. Tier 3 consists of interventions that provide access to therapeutic or other services,[4] which are targeted to students who are already diagnosed with a mental health disorder or who show signs or symptoms of one. Tier 3 interventions do consist of treatment but are also considered preventive in that they aim to prevent greater impairment from mental disorders by managing symptoms.
Table 1
Tiered Framework of School-Based Mental Health Interventions
| Programs/Supports | Target | Purpose/Description | Common Examples | |
| Tier 1 | Universal | All students | School-wide implementation to prevent emotional or mental health challenges | Programs on mental health literacy and awareness, suicide prevention, and social-emotional learning; universal screenings |
| Tier 2 | Selective or secondary | 5%–15% of students | Targeted implementation for students deemed at risk, aimed to prevent emotional or mental health challenges through early intervention | More directed student screening, school counseling sessions; individual and group therapy; further application of Tier 1 programs to more targeted groups of students |
| Tier 3 | Tertiary or indicated | 3%–5% of students | Implemented for students with established conditions or symptoms, aimed to treat and prevent greater impairment | Referrals for individual or family/ caregiver treatment, individualized planning, wraparound services, psychopharmacology, coordinated care for youth with multisystem involvement (juvenile justice, child welfare, etc.), other individualized interventions |
Note: Tiers and descriptions are a heuristic meant to represent the array of school-based mental health services and common examples, though no universally agreed-upon conceptualization or definition for each tier exists among and between education and mental health practitioners; listed interventions are not comprehensive as to what may be used and available in practice.
Source: Table adapted from Krista Kutash, Albert J. Duchnowski, and Nancy Lynn, “School-Based Mental Health: An Empirical Guide for Decision-Makers,” Research and Training Center for Children’s Mental Health, April 2006; and Eric J. Bruns et al., “Fostering SMART Partnerships to Develop an Effective Continuum of Behavioral Health Services and Supports in Schools,” American Journal of Orthopsychiatry 86, no. 2 (March 2016): 156–70
Today, most neighborhood public schools offer some form of mental health programming. Most commonly, these are distinctly packaged Tier 1 programs,[5] delivered by school-employed professionals[6] such as counselors,[7] who also provide one-on-one or group counseling.[8] For example, a school might purchase Second Step,[9] a social-emotional learning (SEL) program, which is delivered by a counselor to teachers or students[10] and consists of activities such as writing down a goal and describing why emotions matter.[11] Tier 2 and 3 interventions are less common.
Tier 1 universal programs that are related to social-emotional development, emotional wellness, prevention, and early intervention are primarily aimed at raising awareness of potential mental health issues, by encouraging attention to emotional states and providing literacy on emotions and mental disorders. The goal is better “upstream” recognition, by teachers and students, of abnormal emotions, behaviors, and mental illness in order to direct more individuals toward mental health services.[12] Theoretically, this should reduce the prevalence of disorders and reduce related adverse symptoms and impacts.[13]
Recent Expansion
Several factors have driven the growth of school-based mental health initiatives in the U.S. in the past half-century. In the 1970s, the public education system became legally responsible for educating children with disabilities, including disability from mental disorders, by providing special education and related services.[14] Separately, mental health policy has come to prioritize attempts to prevent mental illness by promoting wellness and emotional health[15] in society at large. Given compulsory attendance,[16] schools became a natural location for these efforts. Similarly, U.S. education policy has come to place a greater emphasis on wellness because of a perceived relationship between academic achievement and social and emotional development.[17]
The requirement for public schools to provide education and services to those with disabilities from mental conditions is codified in Part B of the Individuals with Disabilities Education Act (IDEA), which provides federal grants to states for doing so.[18] To qualify for funds, local education agencies (LEAs) must locate and identify all children with disabilities regardless of severity, known as the “child find” mandate.[19] LEAs must evaluate whether an identified child is eligible for special education,[20] and provide services determined necessary for the child to benefit from education.[21] For example, for a student with an emotional disturbance (a legally defined disability category),[22] related services may include mental health services, such as counseling,[23] if recommended as part of an individualized educational program (IEP). Occasionally, youth with severe disorders or distress require services outside a typical neighborhood school—including, in more extreme cases, in a hospital or youth residential treatment center—in order to benefit from education. If services in these settings are specified in an IEP, LEAs are responsible for the cost of these placements.[24]
As the focus of U.S. mental health policy has shifted away from providing access to care for those with existing cases of mental illness, and toward prevention and early intervention, the role that schools have come to play as an informal part of the mental health system has expanded even beyond the requirements of IDEA. Schools now often face expectations not only to identify and provide services to those with functional disability from diagnosed disorders but to offer wellness and awareness efforts and to preemptively provide mental health services such as screenings and nonacademic counseling to those facing various social ills and adversity.
Especially in the past decade, school shootings[25] and other troubling metrics of youth emotional distress[26] strengthened bipartisan support for school-based mental health initiatives,[27] and federal funding has reached unprecedented levels.[28] Tier 1 universal programs have been a hallmark of responses to major school shootings[29] since the 2012 Sandy Hook Elementary School shooting in Newtown, Connecticut.[30] The 2022 Bipartisan Safer Communities Act, enacted following the Robb Elementary School shooting in Uvalde, Texas, allocated nearly $1 billion for expansion of such programs.[31]
In education policy, the 2002 No Child Left Behind (NCLB) Act—as well as its 2015 successor, the Every Student Succeeds Act (ESSA)—catalyzed mental health and wellness programming. Both pieces of legislation emphasized a “whole child” approach to education, adopting nonacademic indicators of school success, including, for example, provisions encouraging safe and supportive learning environments.[32] Programs related to SEL, in particular, expanded notably following the passage of ESSA: before the bill, only eight states had some SEL programming, compared with 50 after its passage.[33]
Pandemic-related funding through the 2020 Coronavirus Aid, Relief, and Economic Security (CARES) Act, the 2021 Coronavirus Response and Relief Supplemental Appropriations Act, and the 2021 American Rescue Plan[34] also funded universal programs, as well as initiatives for school-based counseling and capacity building for LEA referrals to outside services.[35] Together, these bills allocated over $1 billion in federal aid to mental health and well-being in schools.
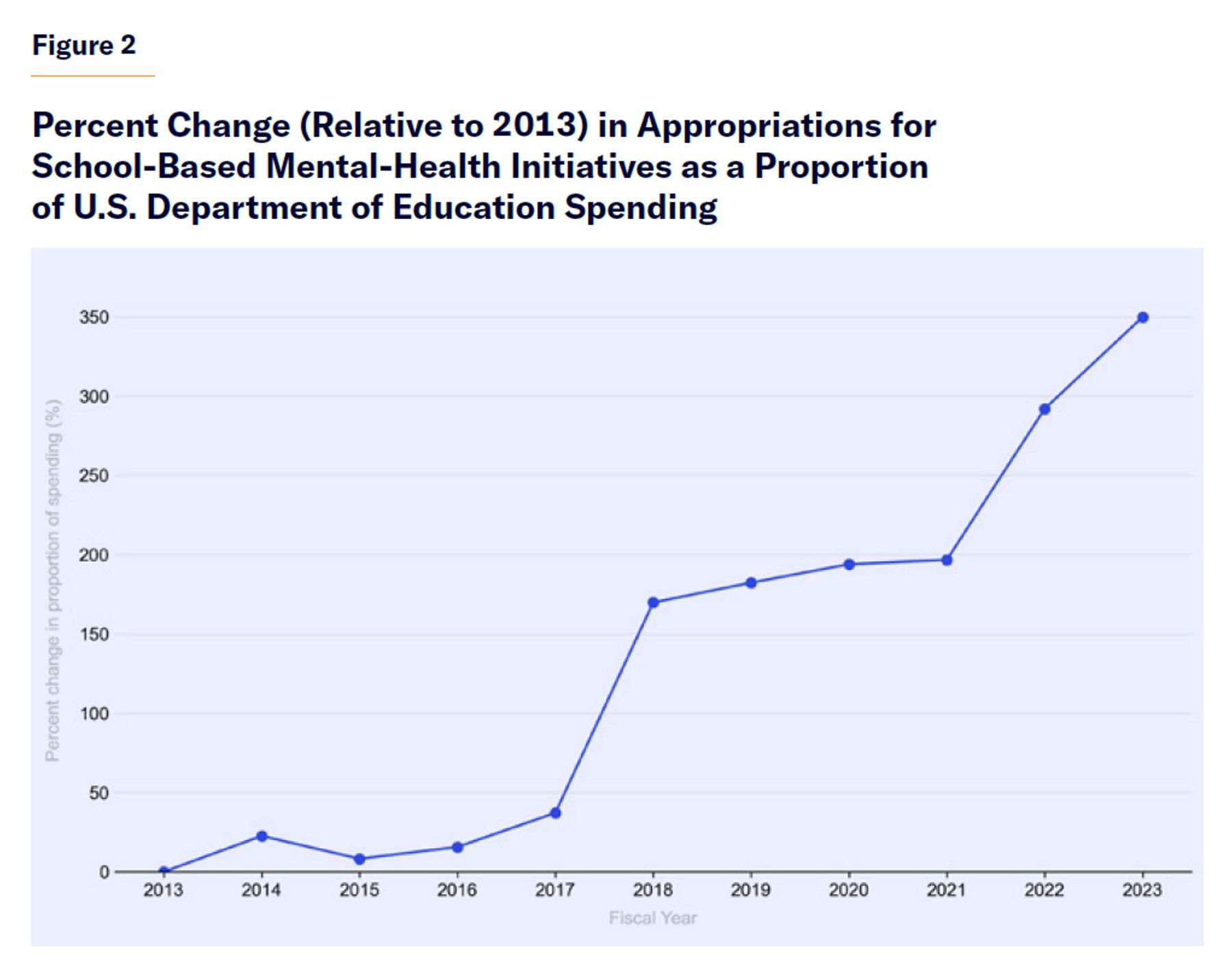
School-based mental health initiatives receive funding primarily from the U.S. Department of Education[36] and the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA), as well as from agencies including the U.S. Department of Justice (DOJ)[37] and through Medicaid.[38] While federal funding for school-based mental health accounts for a small portion of overall spending on elementary and secondary education, Department of Education funding requests for mental health initiatives, in particular, have grown markedly from past years,[39] increasing by nearly 350% as a percentage of overall funding requested for elementary and secondary education (Figure 1; see also Appendix).
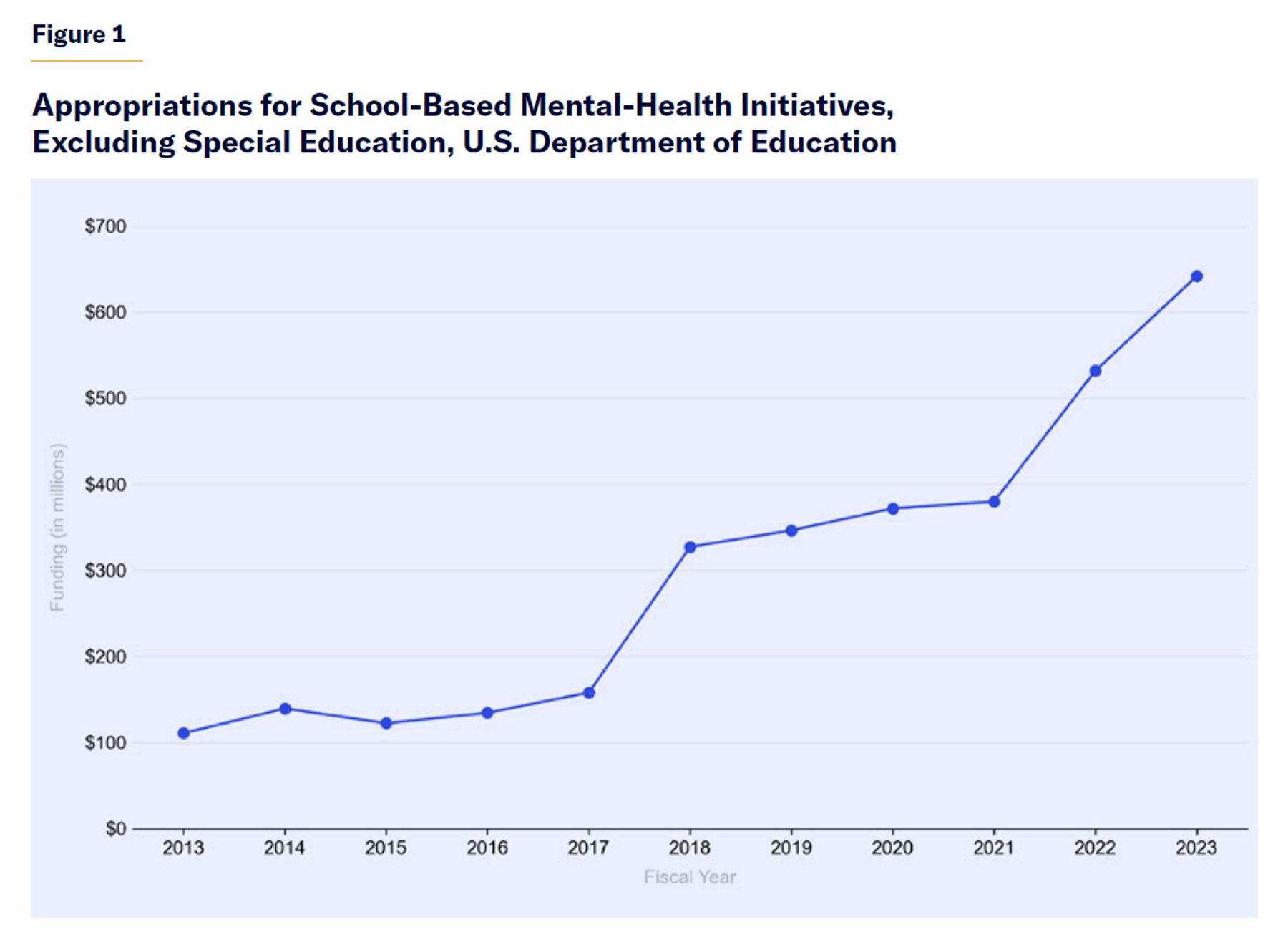
Source: FY 2013–23 Congressional Action, U.S. Department of Education
Notably, states have unique laws and funding streams for various programs, in addition to those required by federal law,[40] though a state-level overview is outside the scope of this report.
Evaluating the Evidence
A sizable literature, established over decades, has evaluated the effectiveness of a wide array of school-based mental health and wellness programs. The results are clear: little rigorous evidence supports universal programs centered on mental health literacy, wellness, awareness, screening, SEL, and prevention as a means of reducing rates of mental illness or disability from mental illness, or to improve academic attainment.[41] Mental health and education authorities historically have a poor track record of successful collaboration, and the implementation of these programs and services has been highly inconsistent.[42] Moreover, serious challenges to delivering mental health treatment via the education system are frequently raised but underdiscussed.[43] Mental health initiatives can place material burdens on schools and educators, who have many competing demands for their time that crowd out academic programming.[44]
Claim: School-Based Services Increase Treatment Access
The strongest argument for school-based mental health initiatives is that they can increase access to mental health care.[45] Empirical evidence supports this claim. For example, a randomized control trial examined the impact of a model in the Minneapolis Public Schools, which, as part of the model, placed clinicians employed by community mental health service agencies in schools, where they could deliver services to students who were often referred by school counselors. The intervention did increase students’ use of psychotherapy.[46] However, increased service use should not necessarily be viewed as a success.[47]
Potential Harm
Mental health treatment has limitations: few effective treatments exist,[48] they are difficult to provide,[49] they are not curative and generally not preventive,[50] and they tend to be less useful for youths than for adults.[51] Clinicians acknowledge concern that treatment carries risk and that expanding access, especially via universal programs, likely has marginal benefit but underestimated potential harm.[52]
Youth who are provided mental health treatment often receive poor-quality service that does not meet established guidelines and best practices.[53] Providers use therapies that have limited or no evidence.[54] Low-income youth are least likely to receive high-quality care.[55] Indeed, even in mental health programs that have been found to improve relevant outcomes, efficacy is highly dependent on the quality of care,[56] which is difficult to measure.[57] And the efficacy of these programs is often lower or erased outside research settings, where they are no longer administered by highly skilled mental health professionals.[58] Students might receive interventions that were evaluated for different conditions or different demographics.[59] Fidelity of treatment constructs are often poorly preserved.[60]
Receiving a mental health diagnosis can influence coping behavior or lead to feeling isolated;[61] diagnoses cannot explain the underlying cause of a disorder because the causes of most mental illnesses are still unknown and poorly understood.[62] Diagnoses can change across providers and over time,[63] potentially causing confusion and helplessness. Some federal, international, and clinical guidance advise against screening interventions—with some guidance specifying that it should be avoided if appropriate referral, diagnostic, or treatment resources are unavailable—because empirical evidence has not demonstrated that screening leads to improved outcomes and because it can induce rates of false positives of over 50%.[64] But this guidance is inconsistent across SAMHSA documents.
Children and adolescents appropriately identified as having a need for mental health intervention have a low likelihood of receiving timely or appropriate care but face higher risk of inappropriately being treated in an emergency department (ED).[65] Youth mental health visits to EDs have increased over the past decade,[66] as have rates of “boarding,” when youth are held in EDs because no appropriately intensive treatment setting is available.[67] Poor-quality mental health treatment can increase risk of self-harm and increase health-care costs.[68] Strong supportive evidence suggests that restricting access to pharmacological agents might also reduce rates of suicide.[69]
There is growing concern about adverse effects from universal programs.[70] Preemptive intervention is associated with worse social-emotional-behavioral functioning,[71] worsening depression[72] and anxiety symptoms,[73] and significantly poorer quality of parent–child relationships.[74] Mental health awareness, for example, has decreased stigma toward some disorders and treatment.[75] But increasing the social acceptability of mental disorders has had the negative effect of normalizing suicidal behavior,[76] pathologizing emotions, incentivizing diagnosis-seeking,[77] and disincentivizing overcoming adversity.[78] Students whose classmates receive a mental diagnosis are at greater risk for later diagnoses themselves, particularly for mood, anxiety, and eating disorders—suggesting that diagnosed disorders might be transmitted via adolescent peer networks.[79] This is in line with evidence showing that social contagion can induce depression,[80] suicide,[81] self-harm,[82] gun violence, bullying, cyberbullying, and violent offending.[83]
Recent reports suggest an increase in teens proclaiming self-diagnosed disorders to teachers.[84] In a poll by EducationWeek Research Center, 85% of students reported using social media to diagnose mental health conditions in others.[85] More students arriving to college have a history of disorders, psychiatric treatment, or psychiatric-related hospitalization.[86] College students who self-labeled as having depression were less able to cope with distress and to plan, had less perceived control over depression, and had more positive attitudes toward medication.[87]
Risk of Overidentification
The most common school-based programs are not direct mental health services[88] but programs intended to direct more youth toward mental health services. But evidence suggests that overidentification (and misidentification) for mental health treatment is common,[89] a problem that school-based mental health initiatives likely exacerbate.
A high proportion of youth identified via universal programs are known cases.[90] IDEA’s “child find” requirement already imposes a federal mandate on school systems to identify all youth with possible impairment from a mental health issue.[91] Some students are identified in targeted screenings that are provided separately in schools and health-care settings.[92] For students not identified in these ways, it is unclear what benefit additional awareness training would provide. In representative studies, adults already recognized symptoms of depression 89.6% of the time[93] and schizophrenia 81.7% of the time,[94] without being taught about the symptoms in mental health awareness programs.[95]
Increased access to mental health treatment through school-based initiatives might have contributed to the overuse of antidepressant and stimulant medications.[96] Referrals to mental health services,[97] as well as diagnoses and pharmacological treatment of ADHD, have been shown to cluster by age, being more common for the youngest students within a grade level—largely as a result of teachers’ pre-diagnostic action.[98] Normative developmental changes might be pathologized by educators and students themselves when viewed in comparison with peers.
Federal guidance in 1991 made special-education services available to students with ADHD diagnoses.[99] Along with shifts in diagnostic criteria[100] and increased public awareness and testing,[101] the expanded youth population considered appropriate for mental health treatment doubled the prevalence rate of ADHD diagnoses among youth from 5.5% in 1997[102] to 11.3% today.[103] The rate of antidepressant use among 12- to 25-year-olds increased 66% between 2016 and 2022.[104] Outcomes measured by morbidity and mortality are not better today than in decades prior.
Teachers may rate students’ social, emotional, and behavioral skills differently based on race and sex.[105] In the late 1990s, the federal formula for special-education funding was updated to address growing concern that a disproportionate number of minority children were identified as disabled, particularly in more subjective categories like emotional disturbance.[106] Adolescents who were referred from schools to a specific federal initiative for mental health services had significantly less global impairment than adolescents referred from mental health settings.[107]
Overidentification is not limited to teachers. Non-psychiatrists have been more likely to diagnose mental health conditions and to prescribe for them than psychiatrists,[108] suggesting some risk to increasing the number of primary-care clinicians in schools or treating mental diagnosis. For about half of youth with a mental health diagnosis, treatment is exclusively a pediatrician-provided stimulant prescription.[109] Stimulant use should be considered with particular caution, as overuse can induce psychosis.[110]
Poor Targeting
To be clear, targeted mental health treatment can benefit some youth with mental disorders. An unexpected drop in adolescent antidepressant use following a policy change saw greater substance use and poorer academic outcomes, particularly among girls.[111] ADHD drug treatment has been shown to reduce risky behavior-related outcomes,[112] hospital use, and interactions with police among some youth with mental disorders.[113] Cognitive behavioral therapy can improve school engagement and reduce criminal-justice involvement for youth with mental disorders.[114] This supports mental health treatment being narrowly provided where there is clear need.
SAMHSA acknowledges that most mental health challenges emerge in late teens to early twenties.[115] K–12 programs are therefore poorly targeted, allocating resources away from areas with the greatest potential benefit. Youth who have serious disorders, and who therefore most appropriately warrant mental health treatment, are some of the least likely to be educated in typical neighborhood schools. But 80% of youth with emotional disturbances do not receive needed mental health services.[116]
Special-education students with a designation of emotional disturbance are included in general education classes less often than other disabled students, and they are also unlikely to receive needed academic support services and family support services.[117] Students with emotional disturbances in a private special-education school who, one year later, were educated in less restrictive educational settings were unlikely to experience success.[118] To the extent that students in traditional public schools need mental health services, it will be more difficult to target those students if resources are allocated to universal programs.
School-based mental health professionals like social workers, counselors, and psychologists often see students facing serious adversity, such as poverty, housing insecurity, neglect, and abuse. In the same way police and judges may “mercy book”[119] adults with mental illness into the criminal-justice system when they perceive no appropriate treatment available except as accessed through the criminal-justice system, school professionals and other clinicians may refer or diagnose students,[120] in an attempt to connect these students with any potential support that can be made available through the education system, including mental health treatment, even if a diagnosis or mental health treatment will not address underlying problems or could unintentionally do harm.
Allen Frances, a prominent psychiatrist who chaired the task force to develop the fourth version of the Diagnostic and Statistical Manual, explains school-expanded access in his book Saving Normal:
In a simpler world, psychiatric diagnosis was once based only on perceived clinical need. But now that it has gained powerful (and unwelcome) influence on many administrative and financial decisions, these decisions have also reciprocally obtained a powerful influence on the rates of diagnosis. Diagnostic inflation is promoted whenever a physician provides an “up-diagnosis” to help a patient gain access to something valuable—like disability benefits or school services. If autism, ADHD, or pediatric bipolar disorder is a prerequisite to being admitted to a small class with lots of individual attention, equivocal cases get shoehorned into these categories, and soon an epidemic is born.[121]
Claim: Mental Health Services Improve Academic Outcomes
Mental illness is negatively correlated with educational attainment,[122] and youth with special-education designations of emotional disturbance experience some of the poorest educational outcomes of any disability category.[123] For youth with mental disorders, targeted treatment and services that help manage symptoms might improve some educational outcomes. For example, justice-involved youth who receive certain types of intensive mental health intervention might be more likely to complete high school.[124]
However, claims that universally administered mental health programs improve secondary outcomes, such as academic attainment, have largely been unsubstantiated by rigorous evaluation.[125] The randomized control trial in the Minneapolis Public Schools, mentioned above, found weak evidence for effects on suspensions or juvenile-justice involvement and no evidence for improvements in average attendance or standardized test scores.[126] Similarly, changes in ADHD drug use have been shown to have no effect on academic outcomes.[127] Greater subsidies for school counselors led to reductions in behavioral problems but had no effect on standardized test scores.[128]
The Collaborative for Academic, Social, and Emotional Learning (CASEL), among the most prominent champions of SEL, has pointed to a meta-analysis reporting that SEL improves academic performance by 11 percentage points.[129] But the meta-analysis comprises studies identified based on arbitrary researcher-chosen keywords and explicitly focuses primarily on positive outcomes. A more rigorous meta-analysis of 56 studies of 38 SEL programs did not find strong evidence that the programs were associated with better academic outcomes, social relationships, emotional well-being, or with problem behaviors.[130] For example, a randomized control trial of the aforementioned Second Step, an SEL program, found no positive impact on academic outcomes and only small improvements in reading and classroom-behavior outcomes when quality of implementation, engagement, and dosage were high.[131]
Conflicting Goals of Education and Mental Health
The shifts in mental health and education policy are, perhaps inconspicuously, fundamental.[132] Until the 1960s, the major emphasis in mental health policy was on treatment and management of individuals with mental illnesses, primarily in institutional settings.[133] In education policy, the primary mission of schools has been to offer an academic education, teaching knowledge and skills like reading, mathematics, and history.[134] While character development and civic engagement have always been present in American public education, the current progressive shift has been toward an individual-oriented therapeutic education, borrowing ideas from pop psychology.[135]
The distinct goals of education and mental health are often in direct conflict. Facilitating mental health services through schools can reduce efficiency, create artificial constraints, distort the system-level understanding of unmet need, reduce clarity for parents on where to seek services, and create greater fragmentation between systems.
School-based mental health interventions replace time spent on academic learning, class prep, and instruction.[136] In one study, 100% of students who dropped out of school counseling did so because they would have needed to miss class and did not want to do so.[137] Teachers and counselors anonymously describe students frequently being pulled out of class for counseling sessions.[138] Teachers express concern that students might use mental health as leverage,[139] or use their counselor’s office as an escape from class.[140] Gradual increases in school avoidance and missed class can put students further behind, exacerbate distress, and create a cycle of greater anxiety toward school.[141]
Some of these therapeutic interventions are promoted as “evidence-based,” but academic impact is not evaluated whatsoever, and an emphasis on emotions might make it more difficult for students to focus on the task at hand.
Attention to wellness has bled directly into academic coursework, even in fundamental areas like mathematics.[142] In one such program, a number-line word problem is adapted to present the situation of a woman owing various amounts of money to others. After students calculate whether she has enough to pay everyone back, they are made to watch a video of a single mother struggling to make ends meet and are asked about how the video made them feel. In one report, a student interviewed after the lesson “broke down in tears when discussing his living situation.”[143]
Data from the U.S. Department of Education show that in the 2021–22 school year, two-thirds of students attended a school with high or extreme levels of chronic absence.[144] Yet 12 states enacted legislation to permit “mental health days” between 2019 and 2022.[145] While chronic absenteeism is at unprecedented levels, it is hard to see how more absences will facilitate better learning outcomes. In addition to absences, mental health awareness also enables more in-school out-of-class time; teachers report pressure to allow students to take walks during class and submit assignments past deadline.[146]
Therapeutic interventions encourage an individual orientation on the part of students, which reduces teachers’ authority over classroom instruction. When educators must enforce classroom expectations and behavior, they risk being questioned by students or parents because it might be “harmful” to a student’s emotional well-being. As a result, expectations are lowered, and fewer tools remain available to maintain order in the classroom. These outcomes make schools less safe and less effective—both of which can increase emotional distress in youth.[147]
Behavioral challenges[148] and staff shortages[149] might incentivize teachers to suggest that parents have their children evaluated for treatment at the first sign of conflict, even when behavior is in line with normal developmental milestones. Accommodations for mental health diagnoses continue to grow; as many as 25% of students at some elite colleges are now classified as disabled, with wealthier students more likely to receive accommodations than poor students.[150] While accommodations might seem beneficial in the short term, they undoubtedly “soften” the world that adolescents confront[151] and are not always associated with improved academic achievement.[152]
To be clear, youth with disabilities that impair their ability to learn warrant accommodations, but policymakers and educators alike should recognize that the goal of normalizing mental health disorders has induced diagnosis-seeking behaviors,[153] which, in the longer term, make individuals less prepared to deal with life challenges.[154]
SAMHSA has made a goal of “promoting wellness”[155]—which it does not define in any useful way but which it does say includes “happiness” and the “absence of stress.”[156] This is at odds with the realities of learning, adolescence, and the human experience.[157] Students asked in a survey to describe how they felt in school most frequently used negative words like fatigue, stress, and boredom.[158] By SAMHSA’s definition, this is a problem. But education should not always induce feelings of happiness; its worth comes not from immediate hedonic pleasure but from the opportunity that it provides to overcome challenges, enjoy successes, and, as one educator described,“learn that a big part of life is doing things you don’t always want to do but that you’re glad you did in the long run.”
When students are met with teachers who encourage them to persevere or who enforce behavioral expectations, they gain useful guidance and perspective as to what constitutes normal life challenges and appropriate emotional reaction and engagement. Students whose emotional responses are validated and excused even when inappropriate might come to see and experience normal challenges as legitimate hardships.
Schools Are Not Clinical Settings
Traditional neighborhood schools are not well positioned to serve most mental health needs of children and adolescents. While schools might feel safe and familiar for students receiving counseling and therapy, they are not clinical or therapeutic settings.[159] School-based mental health services often give rise to ethical challenges around informed consent and clinical competence. Indeed, these programs often operate in a “regulatory gray zone. Mental health records are kept differently than school or primary care records. If the program is sponsored by a community mental health center, it may be required to use certain assessment tools and follow procedures that do not fit the school setting.”[160]
Confidentiality can be compromised because schools do not always have sufficient private space for students to meet with counselors or mental health professionals.[161] School-based professionals face heavy caseloads and time constraints to meet with students, whose levels of need can vary greatly within and across schools. Directly employing mental health providers might even reduce a school’s responsiveness to need. Greater demand for youth mental health services is associated with economic downturns.[162] If need dissipates with economic expansions, schools that have hired mental health professionals will face artificial resource constraint from staff salaries for mental health providers, which could have been put toward longer-term investments such as developing cross-system partnerships with community-based providers.[163]
The roles of school-based mental health professionals, like those of counselors, are often misunderstood, even by direct stakeholders such as teachers, administrators, parents, and students.[164] Counselors do not primarily deliver services such as individual- and group-counseling sessions. Counselors report needing to spend time on non-counseling activities such as clerical work[165] and coworker support.[166] This confusion has contributed to a national shift in the profession from a service-focused model of helping individual students to a program-focused model of “helping all students”[167] (through delivery of mental health programs and training).
Teachers might not understand how to appropriately make referrals, and providers have suggested that school-based services can perpetuate a disengaged “fix my kid” attitude from parents.[168] Nearly 75% of parents believe that their child could benefit from mental health counseling.[169] They might expect or prefer services provided through school-employed counselors even when these are inadequate,[170] because they are convenient[171] or because they are free.
Universal mental health interventions have been criticized as superficial attempts that force teachers to serve as pseudo-therapists even when they are unsure how to appropriately address significant distress and reports of abuse,[172] while also forcing school counselors to serve as pseudo-psychiatrists, who must, for example, evaluate and manage children and adolescents with suicidal ideation.[173] When counselors do provide nonacademic counseling, it is supposed to be initial and short-term.[174]
School-based mental health professionals tasked with doing more than just initial interventions report that what they can or should provide is often inadequate for students with severe disruptive behavior or impairment. During the 2021–22 school year, at least 33% of schools reported that they could not effectively provide mental health services.[175] Most had trouble finding outside providers to whom they could refer students.[176] Too few providers serving higher-need adolescents can have a negative influence on overall school climate.[177]
Evaluating and approving (or denying) a child for mental health services through school can take months and require back-and-forth[178] between administrators, staff, and parents, an expensive process for all parties—and one that is inappropriate for youth needing fast action or considerable intervention. Kristen Eccleston, a special-education expert who led a successful special-education program in Montgomery County, Maryland, describes the processes and procedures as comparable to “deciding what color to paint a lifeboat before sending it to save a drowning student.”[179]
The extensive process for accessing school-facilitated mental health services or accommodations is less problematic for parents who are willing or able to wait for a school’s response because a child’s need is mild compared with a parent whose child’s need is severe. This path is particularly attractive if the time cost of waiting is lower than the financial cost of treatment obtained through the mental health system. Schools wanting to avoid unnecessary administrative burden and possible lawsuits may approve requests for services or accommodations and end up paying the cost. This distorts the market for mental health treatment by allocating more providers and resources to milder cases, where treatment may not have happened if the cost had not been reduced to zero.
For a child whose need is severe, the time cost of waiting for the education system will be highest, as is the financial cost of treatment through the mental health system[180]—if appropriate services are even available. Some 70% of U.S. counties had no child psychiatrist in 2016.[181] In 2023, only 34 states had a single youth psychiatric residential treatment facility, an important care setting for adolescents at risk of self-harm. While high-need students wait for appropriately intensive services and scarce placements to become available, their education is put on pause if they cannot safely be in the classroom.
Ambiguity Reduces Accountability
Vague federal policy has historically hindered successful implementation of well-intended ideas.[182] School-based mental health initiatives are no exception. Federal policy leaves ambiguous the goals and expected outcomes of school-based mental health, the overall costs, the eligibility and scope of programs or services to provide, and the roles and responsibilities of overlapping jurisdictions. Assumed or mandated responsibilities spread across multiple systems convolute responsibilities for all systems. This is a quick way to reduce accountability and lessen incentives to address critical challenges.
A comprehensive assessment of the effectiveness of school-based mental health initiatives on the national level has not been achieved and is likely impossible, given the heterogeneity of programs and services implemented across states, districts, and individual schools.[183] This should concern policymakers from both a fiduciary and an accountability standpoint. Twenty years ago, a typical school would have offered, on average, 14 separate mental health oriented programs.[184] That number has undoubtedly swollen.
Federal guidance describes elaborate considerations for implementing school-based mental health initiatives.[185] Through its Evidence-Based Practices Resource Center,[186] SAMHSA highlights several features as necessary for success:[187]
- A full complement of school and district professionals, including specialized personnel well trained to support mental health needs
- Effective collaboration across families, schools, community partners, policymakers, and providers (who, notably, all face different pressures and goals)
- A thorough needs assessment
- Resource mapping to inform needed supports and services
- A well-coordinated, tiered set of programs and services
- Screening and referral
- Implementation of evidence-based, high-quality practices
- Data to monitor outcomes
- Funding to sustain the school-based system
- Effective leaders[188]
Limitations appear immediately. Most glaringly: nearly all these features distinctly rely on the availability of adequate mental health care providers—but 75% of all rural counties in the U.S. are “mental health deserts” with no providers.[189] Past that, neither SAMHSA nor the Department of Education clarifies what constitutes a well-coordinated, tiered set of programs and services, screening and referral, or evidence-based, high-quality practices.
This guidance does not help schools figure out which programs to select out of the smorgasbord of available options. For example, screenings exist for depression, anxiety, bipolar disorder, eating disorders, PTSD, postpartum depression, early psychosis, and alcohol and substance use, among others.[190] And at least 60 SEL interventions meet ESSA requirements.[191]
Federal guidance also provides little useful or transparent indication about which of the available programs are backed by evidence for improving mental health outcomes.[192] SAMHSA uses the term “evidence-based practice” on its website without defining it[193]—and it does not appear to use the same definition as the Department of Education.[194] ESSA, meanwhile, does not require interventions to demonstrate effectiveness.[195] SAMHSA promotes some programs, such as mental health first aid (MHFA) training, that have touted misleading “evidence”—that is, neither causal nor rigorous and, in some cases, not produced by independent third parties. A highly cited study on MHFA, for example, is of poor evaluation design and is also authored by the program’s creator, who has a direct incentive to claim that it “works.”[196] Many programs are not evaluated for their effect on primary relevant outcomes, such as lower prevalence rates, or reduced disability or impairment from mental disorder.
With respect to “coordination,” should schools provide each separate Tier 1 item of—to name only some—universal mental health screening, universal depression screening, SEL, mental health awareness training, training on trauma-informed practices, suicide awareness training, suicide prevention training, antiviolence programming, and anti-bullying programming?
Does SEL cancel out the need for mental health awareness? Does mental health awareness count as SEL? What conflicting messages exist between any given set of programs? What amount of programming at any tier is adequate? What responsibility does a school have if, through a screening, it identifies a child that meets some clinical definition of a diagnosis, but the student’s education has not been affected? All are questions left to speculation. If the Department of Education and SAMHSA cannot effectively collaborate to plainly define what a system of school-based mental health should do and include, it is not clear how poorly resourced communities can be expected to do so.
Nor do federal agencies concretely define their goals for these taxpayer-funded initiatives. While “mental health promotion”[197] and “doubling the number”[198] of school-based mental health professionals sound positive, what are the expected outcomes of those goals? If promoting mental health is meant to reduce rates of diagnoses—which it may or may not—then taxpayers should not expect that goal to be met by making more providers available to diagnose.
Clear casualties of ambiguity are children and adolescents with the most severe mental disorders. U.S. Senate proceedings during the 2004 reauthorization of IDEA show how distributed responsibility undermines accountability:
The [U.S. Senate] Committee [on Health, Education, Labor, and Pensions] has heard that there is often confusion regarding which public agency has the obligation to pay for children with disabilities who are placed by public agencies in residential treatment or special education schools that are out-of-local agency or out-of-State. Many of these children have multiple and complicated problems, and often are victims of severe neglect, sexual and physical abuse, violence, and abandonment…. [T]he State is responsible for determining which agency is responsible for paying for educational and related services for these children. The committee encourages States to clarify agency financial obligations and responsibilities in these situations, and to make information about those obligations and responsibilities available to school districts and parents of children with disabilities. (emphasis added)[199]
Recommendations
The concept of school-based mental health warrants reevaluation. The wide array of educators, counselors, and aides who support public education consistently face expectations for delivering services beyond academic teaching.[200] Even if it makes sense to “provide a sprawling array of services to students,” writes Frederick Hess of the American Enterprise Institute, it’s “a lot to ask. After all, it’s hard for any organization to do a lot of different things, much less to do them all well.”[201]
Schools are not well suited to deliver mental health treatment effectively. Consider the differences between mental health treatment and treatment for a child with poor eyesight. The latter intervention is relatively straightforward: screening, followed by an eye exam, and provision of eyeglasses.[202] Rarely can mental disorders or distress be addressed through such a discrete path of action.
Children and adolescents facing real adversity—whether from mental disorder or not—merit more substantive support than, say, worksheets asking them to label emotions.[203] Mental health treatment or programming should not be a catch-all solution to wide-ranging adversity just because it is inaccurately perceived as easy to facilitate. First steps by the education system should more closely address underlying adversity in ways that are natural to schools. Anxiety brought on by poor grades, for example, might be better resolved through literacy programs. Depression brought on by a difficult home life might be better addressed through after-school programs that provide a safe environment away from home.
Roll Back Universal Mental Health Programs
Universal mental health programs should not be mandated and should not receive federal subsidies. States that have implemented laws requiring these programs should repeal them or rigorously evaluate their effectiveness; other states should not pursue them. Youth mental health treatment should be pursued judiciously, not universally. Universal programs do not have clear evidence of success, they crowd out time spent on academic learning, and they misallocate limited resources away from targeted interventions to those with known need—a high proportion of whom already do not have access to appropriate treatment.
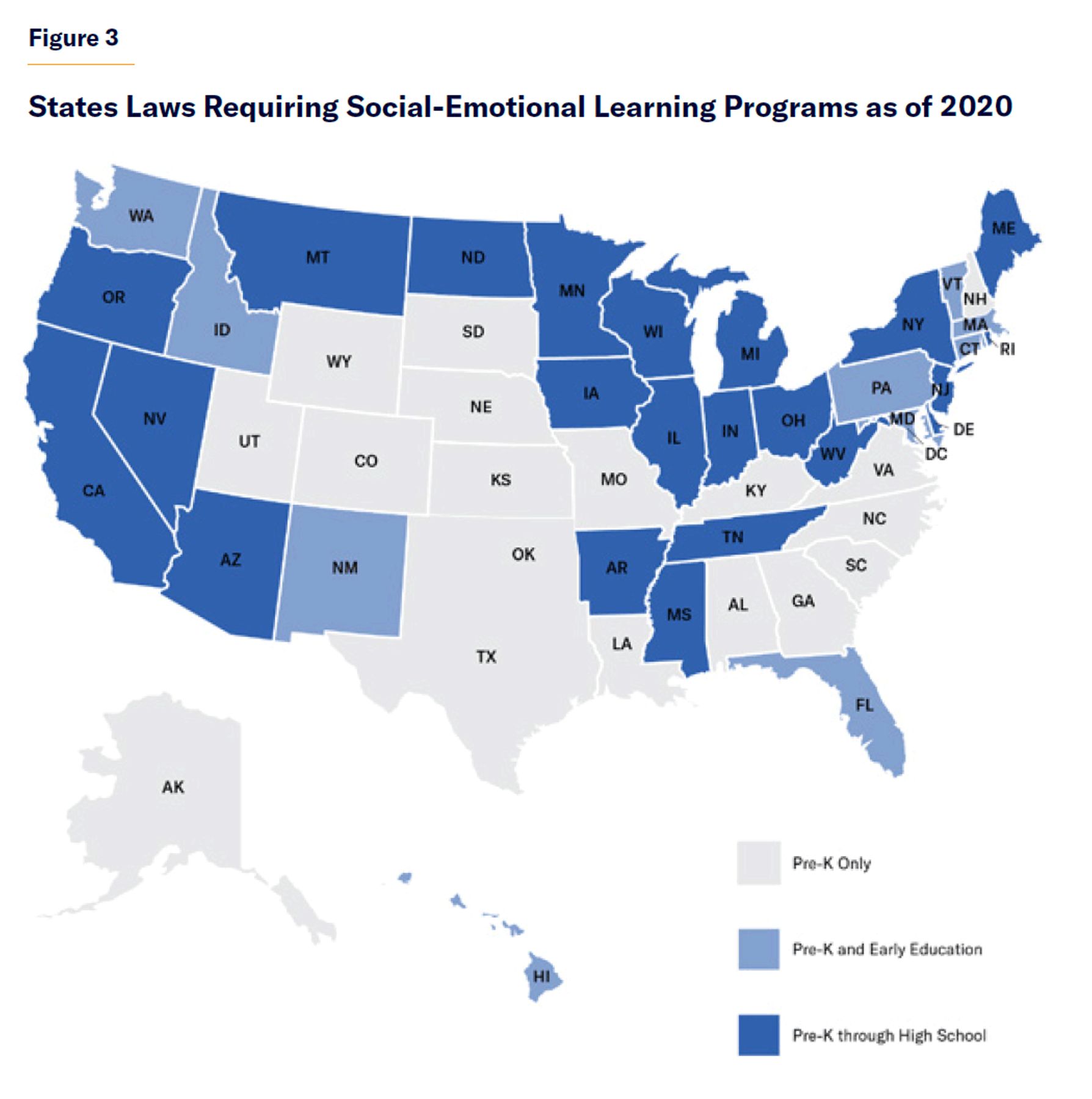
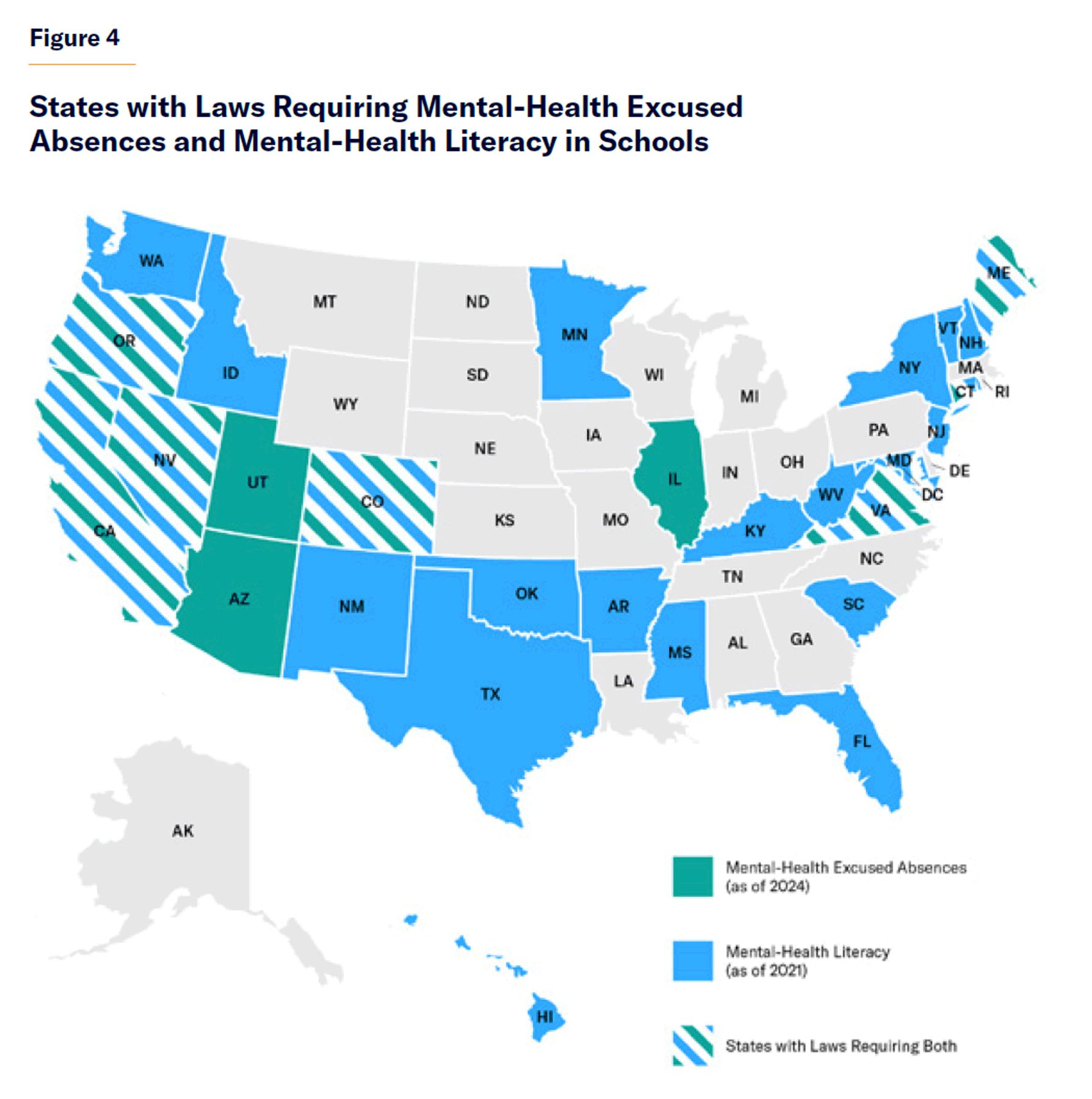
Programs without a strong evidence base include universal applications of mental health awareness training, MHFA, mental health literacy, mental health screenings, suicide awareness training, and many SEL programs. These programs receive funding through specific federal grants and provisions of ESSA.[204] The Appendix includes maps of states that have implemented laws related to mental health literacy and mental health days of excused absences.
Because serious mental health challenges primarily appear later in adolescence, any broad-based mental health programming could be restricted to delivery at the high school level. Given the limitations of youth mental health treatment and associated risks, serious questions should be raised about the age at which youth are exposed to complex concepts such as mental disorder and suicide. Restricting delivery of mental health programs to late teens, when serious disorders can begin to manifest, would reduce risk of harm and better target potentially developing cases of serious disorders. School counselors could and should still be available across all school levels to facilitate academic counseling, provide targeted interventions, and coordinate community-based service access where appropriate.
Renew Focus on Core System Responsibilities
The education system should be allowed to refocus resources on high-quality academic teaching that prepares children and adolescents for productive participation in society. Good academic teaching can improve academic outcomes. Poor academic outcomes can cause emotional distress. Sound mental health policy should therefore support schools’ focus on academic learning. Provisions in federal education law should allow but not require schools to use funding toward school-based mental health. For example, Title IV Part A of ESSA requires that 20% of funds be spent on these efforts, but schools should have more flexibility to address declines in knowledge and skills[205]—particularly important for schools serving low-income children that are often resource-constrained.
In lieu of universal mental health programs and direct hiring of clinicians, schools should implement practices that are structural, relevant to their specific environments, or have demonstrated capacity for implementation in education settings. Structural solutions might include setting schoolwide guidance on behavior expectations and attendance, maintaining full schooldays, keeping doors open after school, and enforcing bans on weapons and, if relevant, bans on phones. Funding now spent on universal mental health programming would provide more value if directed instead toward any of these goals.
Adequately rigorous evidence shows that problem behaviors can be reduced by adopting schoolwide guidelines that define expectations for behavior, provide varying levels of individual support via active instruction and positive reinforcement, and offer a continuum of consequences that minimize reinforcement of problem behaviors.[206] It has also been shown that these positive behavior supports, unlike many mental health programs, can be successfully implemented in schools.
Schools are where youth interact with adults and peers to learn social skills and experience emotional development. So students should be there. Schools should rebuild expectations around full, in-person days—for students, parents, and staff—and maintain fewer arrival and dismissal times. Where possible, keeping doors open after school hours for extracurriculars and additional academic support, such as literacy programs, can provide students with a safe and healthy developmental environment. To discourage school avoidance, states with lower ages of required school attendance could raise that age.[207]
Structural practices like enforcing school policies around weapon bans could lower student distress. Some 75% of members of Gen Z report that mass shootings are a significant source of stress.[208] Research on school phone bans is recent, limited, and mixed, but some studies suggest a small improvement in academic achievement for disadvantaged students.[209] Before mandating school phone bans through legislation, schools at the local level should pursue what is feasible, as success may be dependent on parental support.
Mental health policy should renew focus on the goal of reducing rates of mental disorder and reducing impairment from symptoms by way of providing services to youth with current need of mental health intervention. Promoting “wellness” throughout society has not reduced rates of mental illness. Studies of prevention programs at every level report weak-to-modest effect.[210] Until the causes of mental illness are understood, prevention should not mean universal preemptive treatment but, rather, prevention of the degenerative effects of some severe disorders by means of rapid access to effective psychiatric treatment. Federal mental health funding should reflect as much. First-episode psychosis programs meet this model and are worthy of greater fiscal support.[211]
A first-order responsibility of the public mental health system should be to address high rates of youth with a known need for mental health treatment who receive poor-quality treatment or no treatment at all. State and local mental health agencies can support schools by facilitating partnerships with community-based providers to receive referrals—and, where feasible and warranted, even locate those clinicians in school settings. Clinicians employed by mental health agencies working within schools report fewer competing responsibilities than school-employed clinicians.[212] Locating community providers in or near low-income schools, where transportation to outpatient clinics and costs to patients are of greatest concern, might be worthwhile. School-based providers funded by the mental health system, rather than education-system-funded direct hiring of providers, might clarify expectations and confusion around responsibilities for service provision.
Where no local providers are available, state and federal mental health funding should support increasing access to a full continuum of mental health care. Telehealth might be a viable partial solution for facilitating access to outpatient mental health treatment in “mental health deserts” when appropriate. Efforts to expand telehealth for mental health providers at the state level are ongoing.[213] This solution will be limited to youth who can safely receive services outside a clinical setting and on an outpatient basis.
For some youth with emotional disturbances or high acute distress, more intensive oversight may be necessary. Psychiatric residential treatment can help youth whose educational needs cannot be met in a traditional school setting and whose health is at risk while living in their community.[214] While residential care is a next-to-last resort after more restrictive inpatient hospitalization, it can serve as an important intermediate or transitional setting.[215] Youth psychiatric residential care has seen sharp capacity declines over the past decade, leaving some to languish in emergency departments or some parents needing to send their children out of state for care.[216]
An antiquated federal Medicaid provision called the IMD exclusion should be repealed to remove a financial disincentive to maintain capacity for residential treatment.[217] Residential treatment could also be made exempt from the IMD exclusion to allow for more providers to receive Medicaid reimbursement for services provided. While some residential treatment facilities are exempt from the IMD exclusion through Medicaid’s Psych Under-21 benefit, others are not; onerous and confusing regulations make it difficult to comply with requirements that allow for exemption.[218]
Reduce Ambiguity in Federal Policy and Guidance
SAMHSA and the Department of Education, the two agencies most crucial to delivering school-based mental health services, should define more explicit goals for school-based mental health and assess those goals with meaningful outcome measures. Guidance should have greater specificity as to what constitutes a program as effective and worthy of funding support. The ambiguous policy goal of “promoting wellness” should be discarded, as there is no realistic way to evaluate success. The goal of “preventing mental illness” has not been met through this prevailing approach. To the extent that school-based mental health initiatives are meant to decrease rates of diagnosed mental disorder and increase access to treatment, those two goals alone may be in conflict with anything other than service provision to already-identified youth.
At a minimum, federal policy and guidance should provide a clear and meaningful definition of what it means for a program to be “evidence-based” and set an appropriately high bar for meeting that definition before supporting or recommending a given program. Interventions should be assessed on directly relevant and meaningful outcome measures such as reduced prevalence or impairment of mental disorders. Programs should also have a demonstrated capacity for consistent successful implementation specifically in school settings to be supported for school-based deployment.
Acknowledgments
The author would like to thank Kristen Eccleston, Sarah Nazarian, Polly Gannon, Cristiana Dobra, Melissa Johnson, Samantha Harrison, Emma Shuman, Rory Foster, Jim Kucko, Carissa Schwarzlose, and other school-based professionals not named for their valuable perspectives directly working to help students at the individual level. The author would also like to thank Stephen Eide, Ray Domanico, Brandon Fuller, Sherry Glied, Danyela Egorov, Kevin O’Connor, Max Eden, Andy Smarick, Vincent Schiavone, Scott Dziengelski, and Dia Jackson for their insights, and Santiago Vidal for his research assistance.
Appendix
Source: FY 2013–23 Congressional Action, U.S. Department of Education
About the Author
Carolyn D. Gorman is a Paulson Policy Analyst at the Manhattan Institute where her research examines how policy changes in the U.S. impact individuals with mental illness. Previously, Gorman was a data science and policy associate at the JPMorgan Chase Institute, an associate research scientist at the Coleridge Initiative, and the senior project manager for mental illness policy at Manhattan Institute. She served as vice chair of the board of the former Mental Illness Policy Org., a nonprofit founded by the late DJ Jaffe, and as staff on the U.S. Senate Committee on Health, Education, Labor and Pensions.
Gorman’s writing has appeared in the Wall Street Journal, New York Daily News, New York Post, City Journal, National Review, The Hill, and RealClearHealth, as well as the peer-reviewed Psychiatric Services and The Routledge Handbook of the Economics of Ageing. Gorman holds a B.A. from Binghamton University and an M.S. in public policy from the Robert F. Wagner Graduate School of Public Service at New York University.
Endnotes
Photo: Stephen Welstead / Stone via Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).