The Tradition and Limits of Campus Mental Health

Photo: Noko LTD/E+ via Getty Images
Executive Summary
Campus mental health services are rooted in distinct Progressive-era movements that sought to improve individuals and society through psychological and psychosocial interventions. Campus mental health services, which predate today’s “mental health crisis” framing, have failed to produce aggregate improvements to well-being, intellectual development, or civic formation.
While campus mental health services center around counseling centers, such centers are not historically medical in nature and do not have a single theory of excellence or unified purpose; in these ways, they are subject to the ever-changing needs of students who elect to use services, without knowing what services will be needed.
Campus mental health services, as currently implemented, are better understood as a student experience amenity more so than health care. The expansion of these services, therefore, should not form a part of higher-education reform efforts aimed at improving economic returns, civic preparation, academic rigor, and intellectual diversity.
Further, institutions should consider potential ADA exposure and discrimination liability before expanding mental health programming and oversight beyond what is required to provide.
Introduction: The Historical Development of Campus Mental Health
Campus mental health services—as well as the professional counselors who often provide these services[1]—largely evolved out of two complementary Progressive-era movements: the mental hygiene movement; and the vocational guidance movement. Both sought to apply professional expertise to improve societal well-being through psychological interventions.
The Mental Hygiene Movement
The early-20th-century mental hygiene movement was an attempt to develop preventive mental health care.[2] The movement drew its theory (and the term “hygiene”) from public health, which was a popular model following the great success of sanitary reform.[3] Adherents of the mental hygiene movement theorized—though never proved—that serious mental illness was the result of distress from normal life challenges and poor social environments. Mental illness could thus be prevented through improving mental hygiene—which included environmental manipulation (e.g. advocating for government assistance to improve social conditions), education on well-being, and early (preemptive) psychological treatment[4] in the masses.[5] Particular emphasis was placed on children and young adults.[6] A fairly deliberate and aspirational shift in terminology to mental “health” from mental “hygiene” was later made because the movement was deeply entangled with eugenics.[7]
Prior to the mental hygiene movement, the primary job of psychiatrists and psychologists was to treat active cases of mental illness (which was more narrowly defined).[8] In its wake, treatment of active cases was de-prioritized in favor of large-scale prevention efforts. The movement has profoundly shaped mental health policy on- and off-campus, and its ideas continue to dominate: we say “mental health” policy, not “mental illness” policy. Mental health professionals today spend far more time on every day “problems of living” than they did in the century prior,[9] despite the failure of a public-health approach to prevent mental illness. In the process, many of these regular problems of living have been redefined as clinical diagnoses—mainly for altruistic reasons—to expand service access through insurance coverage and eligibility for public benefits.
In all likelihood, the first campus mental health service was a small mental hygiene clinic at Princeton University, established in 1910 by psychiatrist Stewart Paton.[10] A mental hygienist, Paton argued that colleges were not preparing students to handle the stresses of modern life, which he believed could lead to their developing “shell shock” like that seen in soldiers. Concern over the psychological vulnerability of college-age men (and the implications for military readiness) motivated the creation of clinics at other institutions.
Also influential was University of Chicago, which recruited prominent psychologist Carl Rogers in the 1930s to create a counseling center for students.[11] Rogers is well-known for developing client-centered therapy, or client-centered counseling, a nonjudgmental style of psychotherapy based on supportive listening. The primary goal of the client-centered therapist was to reassure clients that their feelings were valid, that they felt heard, and that they experienced themselves as received.[12] Rogers described the Chicago center’s work as adjustment counseling, dealing with students struggling to adjust in social or academic contexts.[13] Rogers’s prominence in the field of psychology and work at Chicago raised the profile of campus counseling.[14]
Over the following decades, a minority of campuses began to incorporate clinical and psychiatric treatment services with a medical-model orientation, which had grown in prominence, culturally.[15] These campus services, provided by psychiatrists and clinical psychologists, primarily screened for serious psychiatric conditions such as schizophrenia and bipolar disorder.[16] But the mental hygiene tradition—of prevention, mental health education, and early psychotherapeutic intervention—maintained centrality. Campus counseling centers, developed in part to provide vocational guidance, expanded to offer “personal adjustment counseling” to help students adjust to campus life and adulthood.[17]
Vocational Guidance and Counseling Services
Today’s campus mental health services apparatuses can also be traced to a separate but parallel trend: vocational guidance, the precursor to counseling,[18] which emerged as a field of psychology in the early 1900s to help young people navigate the growth of college curricula and career options in the era of industrialization.[19]
Educational and vocational counseling centers became more common on campus after World War I, when psychologists adapted psychological testing techniques originally developed for the U.S. Army for use in student services.[20] Across the country, schools began to implement a model of psychometric assessment and career and educational counseling, emphasizing a “student as a whole” approach to personal development that sought to help students discover “multipotentiality” and increase “life satisfaction.”[21]
Throughout the 1930s, these types of counseling centers proliferated on campus, under a variety of names. These centers were not focused on mental illness. They were typically located within academic affairs, and had an educational, not medical, orientation. As described in History of College Counseling and Mental Health Services and Role of the Community Mental Health Model:
[S]tudents in the early 1900s received support from a variety of individuals who called themselves “counselors,”“advisors,”“student personnel workers,” “vocational guidance workers,” or “mental hygienists.” This eclectic group of individuals described helping students with educational, vocational, financial, moral, and personality problems that interfered with students’ academic progress.… As quoted [by one observer] in 1936, “the psychologist, the physician, the psychiatrist, the mental hygienist, the sociologist, for that matter the butcher, the baker and the candlestick maker, each took his turn at claiming … that he was the one and only individual to deal with student problems.”[22]
Post–World War II Expansion and Professionalization
Campus mental health dramatically expanded after World War II, largely because of the 1944 GI bill.[23] In addition to paying veterans’ tuition and living expenses, the bill provided a benefit for educational-vocational counseling.[24] To facilitate this benefit, the Veterans Administration (VA) contracted with 25% of all colleges and universities to create on-campus counseling centers, fully subsidized by federal funds.[25]
By 1951, these centers had counseled 2.5 million individuals,[26] which may have been considered by some to be evidence of their success, regardless of whether individuals counseled saw better outcomes. Some VA studies claimed that the program benefited taxpayers because students who opted to receive counseling were less likely to switch to a different educational and vocational training program than those students who did not opt to receive counseling. But it is not clear that these studies accounted for fundamental differences between the groups. Further, it was a benefit insofar as a new public spending program may have cost less than could have been paid for it. After federal subsidies expired, most schools maintained their counseling centers and others began to establish them.
The 1950s saw the formalization of distinct counseling professions, formed out of the proliferation of many schools of psychological theory and approaches of the earlier half of the century. A landmark 1951 conference helped establish the “counseling psychology” profession, which was differentiated from psychiatry and clinical psychology by its focus on “individuals within the normal range” rather than on mentally ill patients.[27] Counseling psychologists integrate vocational guidance, assessment, and psychotherapy while psychiatrists and clinical psychologists use a medical model of mental illness, which de-emphasizes social and developmental factors as causal. In the 1980s, several new types of distinct counseling programs were accredited, primarily located in colleges of education and generally focused on day-to-day life management and talk therapy.[28]
The formalization of the counseling professions involved several accreditation bodies and professional organizations. The International Association of Counseling Services (IACS)[29] became the main accreditation body for counseling centers, while the Joint Commission on Accreditation of Healthcare Organizations (JACHO)[30] accredited student health centers, including psychiatric services. The Association for University and College Counseling Center Directors (AUCCCD, established in 1950)[31] and the American College Counseling Association (ACCA)[32] served counseling center professionals, and the American College Health Association (ACHA, established in 1920)[33] served professionals in student health centers.
Counseling centers emphasizing developmental, educational-vocational, and preventive approaches historically have dominated. These centers are rooted in Progressive-era faith that social problems could be solved prophylactically: the mental hygiene movement promised that early intervention could prevent mental illness and produce happier, more civically engaged, Americans. Vocational guidance believed that matching individuals to majors and careers based on psychological assessment would benefit workers as well as society. While both sought to help individuals manage and adjust to their social-environmental context, proliferation of approaches in psychology and counseling—in some sense, in an altruistic entrepreneurial manner by psychologists and counselors—mean that counseling centers did not develop a single shared vision for what the center was or should be. Regardless of their creators' intent, counseling centers were subject to whatever challenges the students who came in to use them faced.
The Modern Campus Mental Health Apparatus
Although few attempts have been made to quantitatively survey the array of mental health and psychiatric services currently offered across institutions of higher education (IHEs), counseling centers that promise to help students with general life challenges remain a core offering.[34]
Counseling Center Personnel and Services
Cross-sectional data from 2025 of descriptions on IHE websites show that nearly all offer some form of mental health services, with counseling as the most common descriptor.[35] Fully 95% of two- and four-year institutions, 80% of community colleges, and 99% of institutions with at least 1,000 students report offering such services. In surveys, the vast majority of college presidents report that their institutions provide mental health services.[36]
To receive accreditation from IACS,[37] IHE counseling centers must provide:
- individual counseling for personal adjustment, vocational, developmental, or psychological problems
- crisis intervention and emergency services (though they may be contracted out)
- “preventive programming” (e.g., to help students “acquire new knowledge, skills, and behaviors; encourage positive and realistic self-appraisal”; and “enhance the ability to relate mutually and meaningfully to others”)
- consultation and outreach to the university community
- referral resources for students whose problems are outside the scope of counseling center services
- regular evaluation of counseling center services
- while not a center requirement, psychiatric services also must be provided either on campus or be available in the community.
To learn more about what is needed for these centers to operate effectively, AUCCCD surveys its members annually. Although the responses may not be perfectly representative, they offer insight into the structure, staffing, and offerings by the subset of respondents.[38]
In the most recent survey (covering the 2023–24 academic year), the vast majority of responding directors were at four-year institutions (88%) and at multi-staff counseling centers (98%). The average number of full-time-equivalent counselors per center was about nine at four-year institutions and five at community colleges. Directors were disproportionately female (73%), and 30% identified as a person of color, up from 16% in the 2012–13 survey. Some 17% were LGBQ+-identified, as compared with 9% in the general population, and 1.3% identified as outside the gender binary.[39]
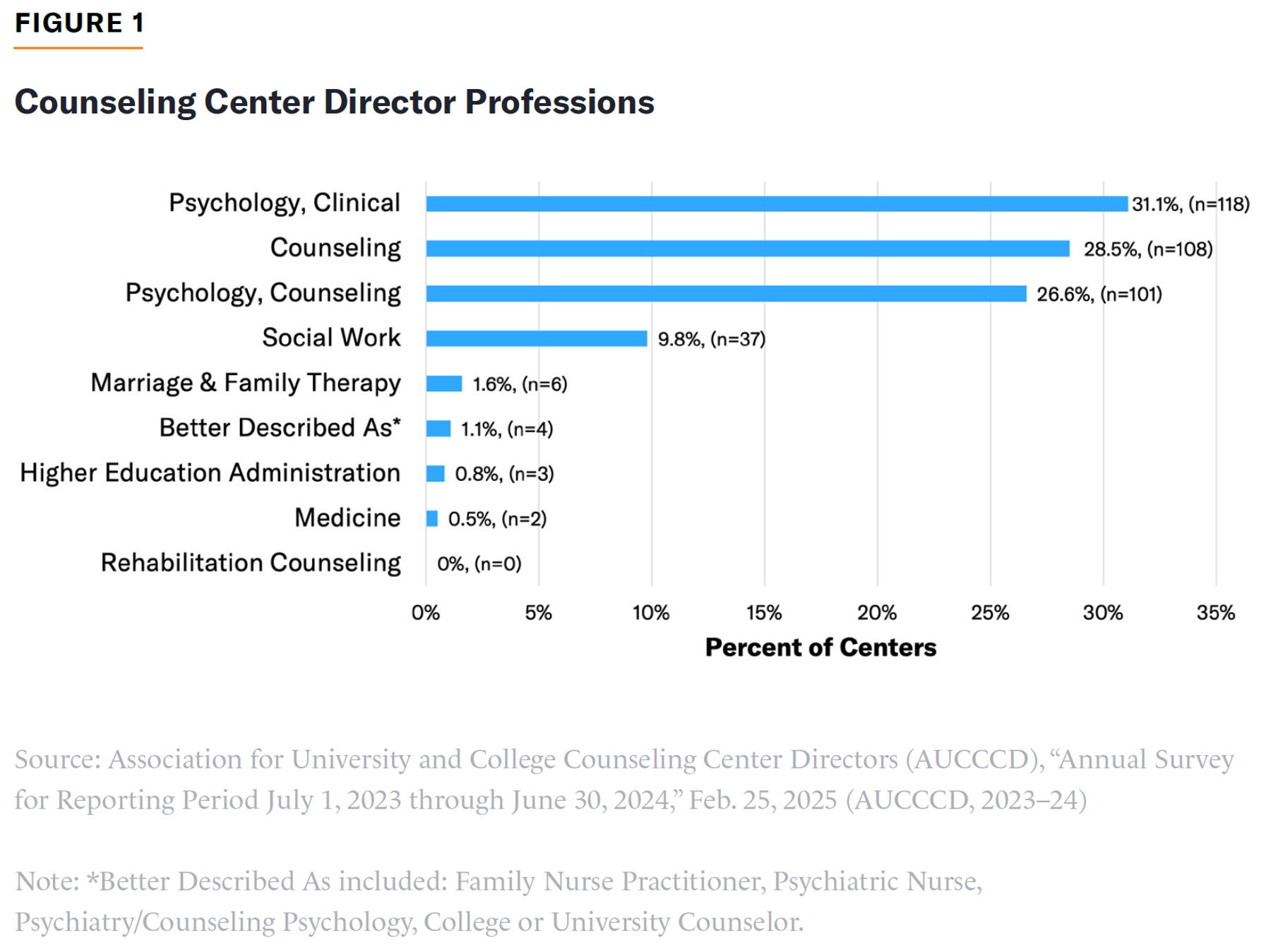
As shown in Figure 1, fewer than one-third of directors described their profession as clinical psychology or medicine (which are most indicative of psychiatric and medical services). More than two-thirds described their profession as counseling, counseling psychology, social work, or marriage and family therapy—all of which are more likely to involve talk therapy for students with normal distress levels. Per AUCCCD, talk therapy involves one-on-one sessions that do not include triage, screening, intakes, psychiatric, or crisis appointments. Although not shown in the figures, 60% of directors held a Ph.D. or Psy.D. but only 0.5% held an M.D.
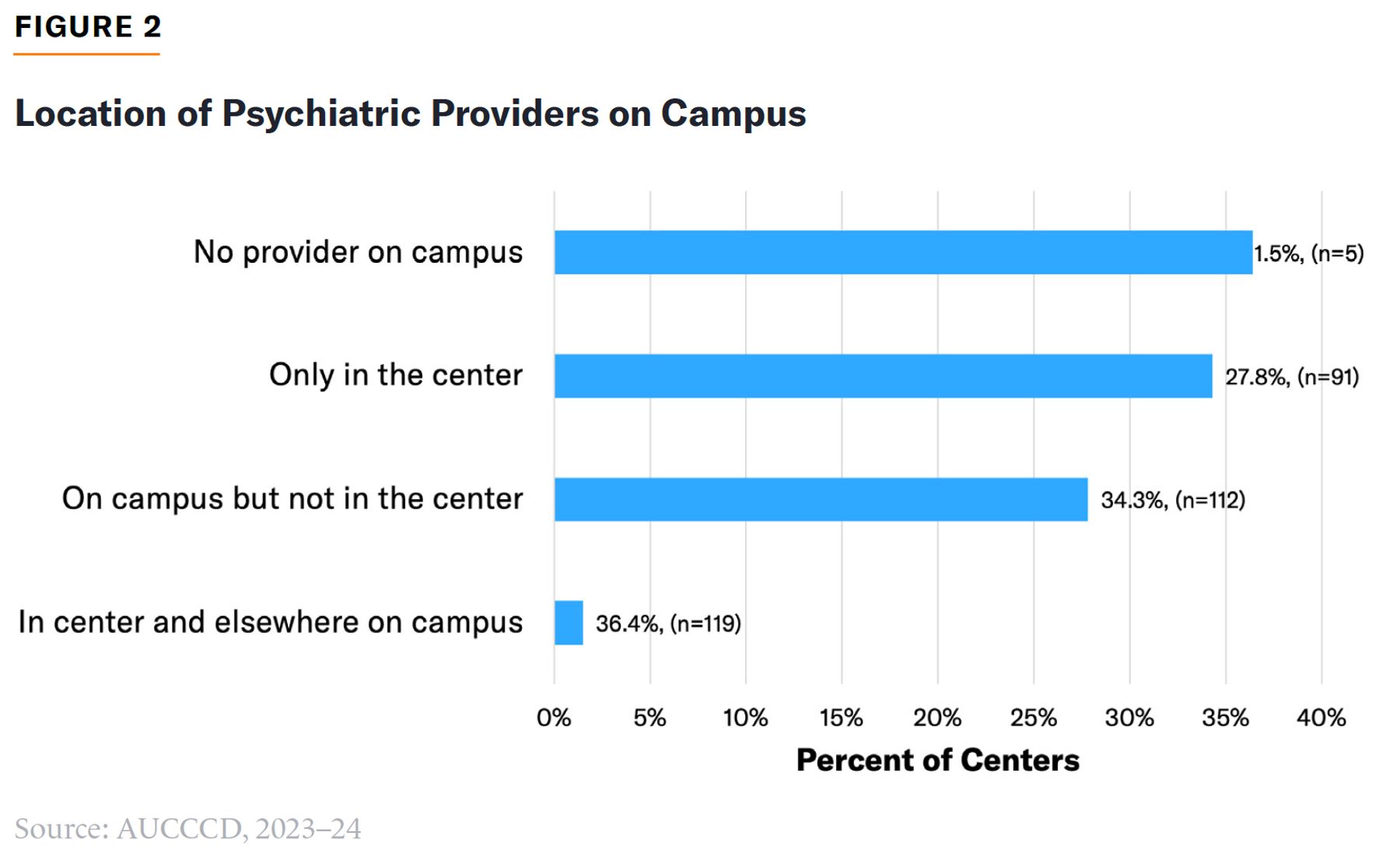
Nearly two-thirds (64%) of directors report that psychiatric services are not provided on campus or are provided on campus but not in counseling centers (Figure 2).
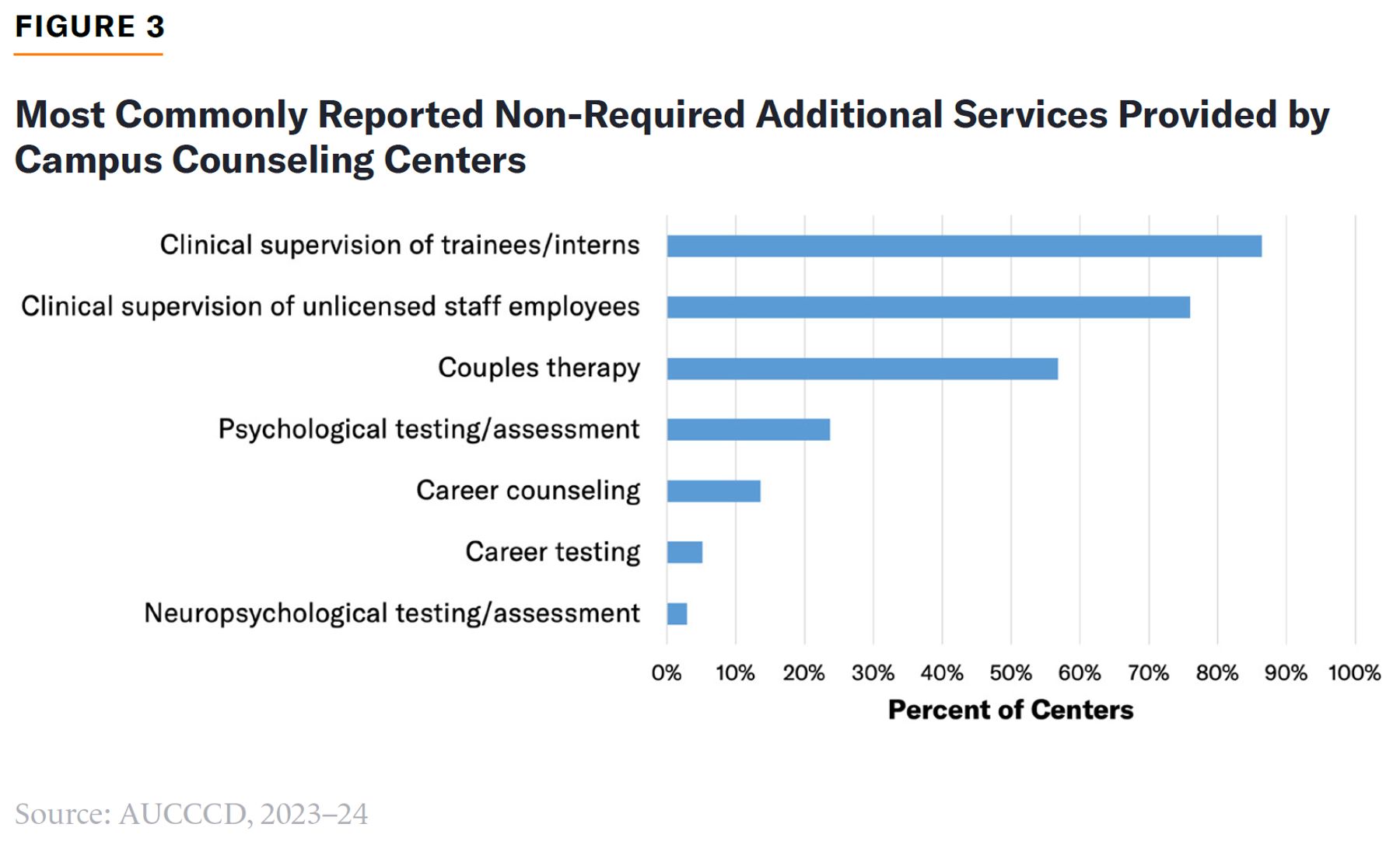
In addition to required services described above and group therapy, responding directors most commonly reported providing clinical supervision of nonclinical staff, couples therapy, and psychological testing and assessment (Figure 3). Fewer than 20% of directors reported providing career counseling or career testing.
Counseling centers serve a minority of the student body. Respondents at four-year institutions reported, on average, that 11% of students received at least one service of any type from the counseling center; at community colleges, the figure was just under 5% of students. Counseling centers at smaller institutions (≤2,500 students) served a greater portion of the student body on average (8%–19%), compared with 6.5%–8.1% at large institutions (>45,000 students).[40] Because smaller institutions are disproportionately rural, this may be a result of a difference in the availability of various off-campus health, mental health, employment, and social services.
At some schools, a disproportionate share of services may go to a small number of “power user” students. Research from the Center for Collegiate Mental Health at Penn State University finds that 20% of all clients served by counseling centers accounted for 57% of all appointments.[41] AUCCCD finds that the average number of sessions per unique student is about five. Likely, a typical student receives only a handful of sessions, and meaningful variation exists around that typical experience. Separate research suggests that the symptoms most predictive of on-campus service utilization are alcohol-use disorder, followed by depression and stressful life events.[42]
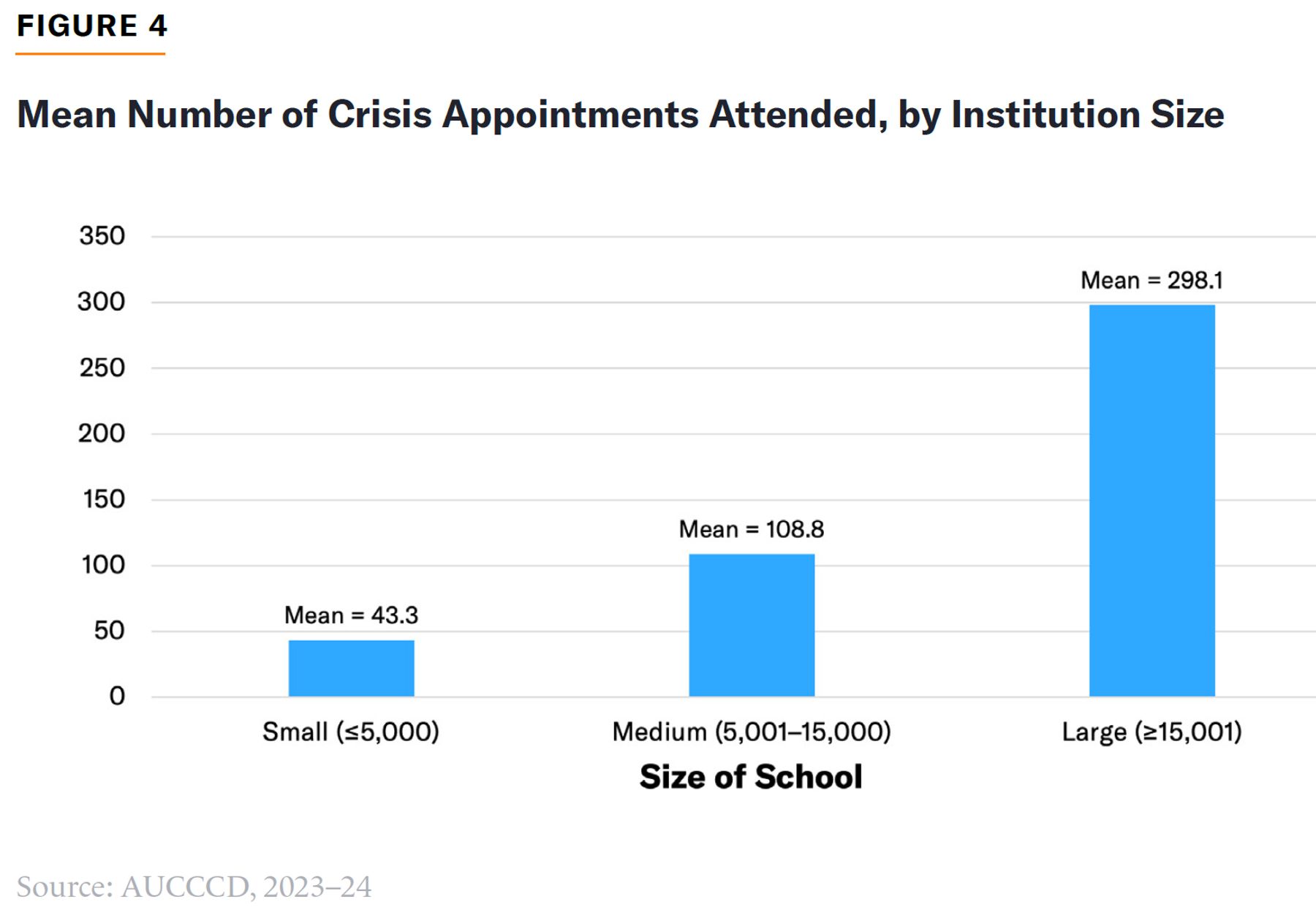
AUCCCD data show that very few students attended a crisis appointment in 2023–24 (approximately 125 visits per center), but it is unclear whether this figure represents the number of unique student visitors per center (Figure 4). Further, most centers used a third-party vendor or a community hotline for crisis services. Possibly, many counseling centers are unable or unwilling to offer crisis services.
Campus-Wide Wellness Initiatives
In the past decade, particularly since the Covid-19 pandemic, campus-wide wellness initiatives promoting mental health have expanded. These efforts are frequently facilitated by or offered by counseling centers. Such efforts include campaigns promoting self-care, encouraging positive mindsets, creating psychologically welcoming environments, and supporting the spirit of diversity, equity, and inclusion.
Many IHEs offer designated wellness or relaxation spaces[43] and services like pet therapy to help students de-stress.[44] University of Michigan offers 17 “reflection rooms”[45] and a “wellness zone”[46] with massage chairs and light therapy. Before the 2024 election, the University of Oregon offered animal therapy sessions with a duck.[47] The State University of New York (SUNY) system, in 2022, used $24 million in federal funds from the American Rescue Plan to hire a diversity officer focused on the mental health of diverse populations and create a diversity mindfulness room for “BIPOC” students.[48]
Many institutions have embraced mental health awareness training curricula, the most popular version of which operates under the brand name Mental Health First Aid. In 2021, the University of North Carolina established a goal of training 10,000 people in Mental Health First Aid, which it accomplished in 2025.[49] In 2022, Maryland launched an initiative to train 20,000 students, faculty, and staff at the state’s four historically black colleges and universities (HBCUs).[50] Beyond formal mental health awareness training programs, the idea of promoting mental health via education about how to recognize distress has spread. IHEs in Texas, as of 2023, are required by state law to offer entering students information about early warning signs of suicidal ideation.[51] Indiana University’s “Unboxed” campaign encourages students not to “box up” or suppress internal struggles and, rather, to reach out and open up to the university, “an ally,” in their experience.[52]
Legal Obligations for Students with Mental Health Disabilities
IHEs face two primary federal legal obligations regarding students with mental health disabilities: Section 504 of the Rehabilitation Act of 1973, which prohibits discrimination by institutions receiving federal funds;[53] and the Americans with Disabilities Act of 1990 (ADA),[54] which extends protections to public (Title II)[55] and private (Title III)[56] institutions, regardless of federal funding status.
No federal law requires institutions to provide mental health or psychiatric services. Disability law requires reasonable accommodations for students with disabilities and prohibits discrimination. Under ADA, mental health conditions qualify as disabilities when they substantially limit one or more major life activities[57] (for psychiatric diagnoses, such activities might include, for example, thinking, learning, concentrating, communicating, sleeping, and interacting with others).[58] The statutory language defining mental health conditions is intentionally broad, and specific or explicit conditions need not be listed within the statute to qualify.[59]
The ADA Amendments of 2008 (ADAAA)[60] significantly broadened coverage by establishing that “substantial limitation” is “not meant to be a demanding standard” and that episodic conditions and those in remission qualify. Amendments also barred consideration of mitigating measures, such as treatment and medication, when making disability determinations. In other words, students who are already effectively managing symptoms through treatment remain protected under ADA. The amendments extended ADA protection to individuals with a record of mental health impairment or diagnosis (including those misdiagnosed), even if functional limitation criteria are not currently met.
Reasonable accommodations might include extended exam time, modified attendance or leave policies, reduced course loads, and housing.[61] IHEs may not exclude, suspend, or pressure a student to withdraw solely because of a mental health diagnosis or suicidal ideation, unless the student poses a direct threat that cannot be mitigated through accommodation.[62] ADA prohibits “zero tolerance” policies that require automatic withdrawal for students who express suicidal ideation.
Importantly, in addition to protecting those with documented disabilities, ADA also contains a provision that protects those who are “regarded as” having a disability, meaning an individual need not have a disabling condition to be discriminated against; an individual need only show that an institution took an adverse action against them because the institution perceived them as having a physical or mental impairment. For example, an institution that flags a student for mandatory mental health evaluation, places them under a behavioral monitoring program, or restricts their participation in normal activities on the basis of a perceived psychological risk has, in doing so, treated them as disabled within the meaning of the statute. The adverse action itself is what triggers coverage under ADA, not any underlying clinical diagnosis or disability designation received after an accommodations request.
This distinction has practical consequences. ADA discrimination claims arising under the “regarded as” prong do not require proof that the institution failed to provide a reasonable accommodation. Accommodation obligations attach to individuals with current, or a record of, disabilities who request modifications to participate in a program or activity. Discrimination claims, by contrast, require only that the institution treated the individual adversely based on a perceived impairment. In practice, this puts institutions at risk of legal action for using some tools that may be appropriate and useful for maintaining student safety. Consider a student seeking to return from a leave following a suicide attempt. If the university mandates psychological clearance before the student returns to class, the institution may have engaged in discrimination.
One implication of this: the broader and more systematically an institution applies mental health frameworks to its population, the broader the class of individuals it may be “regarding as” disabled and the greater its potential liability for any differential treatment that follows.
There is a fundamental tension between these antidiscrimination measures and a university’s “duty to protect” students from harm, including suicide. In recent years, several state supreme courts have ruled that universities have a special relationship with students, giving rise to a duty to protect students from foreseeable harm when on campus or engaged in university-sponsored activities.[63] This creates potential tort liability: institutions may face lawsuits alleging failure to prevent foreseeable harm, including student suicide. Suicide attempt and outwardly-directed aggression are associated.
Federal disability law constrains institutions’ traditional approaches to student safety, including mandatory psychiatric evaluations as a condition for continued enrollment or return, involuntary medical leave, or mandatory withdrawal when students disclose suicidal thoughts or self-harm. Under ADA, colleges may exclude a student who poses a “direct threat”—defined as significant risk to the health or safety of others[64]—after conducting an individualized assessment based on objective evidence. But regulations notably omit “threat to self” from this definition, creating legal uncertainty about intervention for students at risk of self-harm.
Assessing Outcomes, Utilization, and Concerns
Campus mental health services have existed for over a century, with particularly notable expansion especially over the last several decades. But overall student well-being and aggregate academic outcomes have not improved. Both, in fact, are worse today than in decades past.
Proponents of campus counseling claim that the practice is justified financially: counseling can prevent students from dropping out,[65] which prevents the institution from losing tuition dollars.[66] The empirical evidence for this argument is mixed. Some point to self-report surveys of counseling center clients who say that the services help them stay in school, but these surveys suffer from sample bias and are not empirically rigorous.[67] Other studies suggest that individual counseling for struggling students can help prevent dropout among first-year students[68] or can do so when targeted to students at high risk of dropout.[69] An evaluation of a 12-week counseling intervention designed to address mental health and academics had positive impacts on self-referred, at-risk students.[70] Again, however, self-referred students may differ in fundamental ways from those who do not seek or want help. Financial justification for providing services also must be weighed against the financial liability that may be associated with offering those services.
Expanding mental health services does not guarantee that students will receive appropriate care, or that care will improve academic outcomes.[71] In one study of community college students, engagement with campus resources was not significantly related to persistence.[72] Among unprepared college freshmen, failing remedial courses—rather than access to services—was the most significant predictor of enrollment retention.[73] A review of randomized controlled trials, a gold-standard evaluation design, related to online mental health interventions found no significant effect on academic outcomes and only a small effect on depression.[74] Among mentally distressed students aware of campus services, some chose not to use them.[75]
While it has long been known that mental health conditions are associated with lower rates of educational attainment, higher dropout rates,[76] and other adverse life outcomes,[77] this research often focuses on disorders that emerge before, or independent of, college. Further, the overall dropout rate among college students is only 5.3%, a small share to justify large-scale mental health efforts.[78]
Campus counseling centers do not have a clear, uniform purpose or goal. Because they developed out of a proliferation of approaches within various schools of psychology, they lack a shared vision of excellence. Counseling centers also have to adapt to changing cultural challenges faced by students. In one way, counseling centers are similar in what they are not: they are generally not medical service providers for students with the most acute psychological or psychiatric needs—who are at highest risk of dropping out for reason of mental health. Those students are least likely to be served adequately by existing campus services.
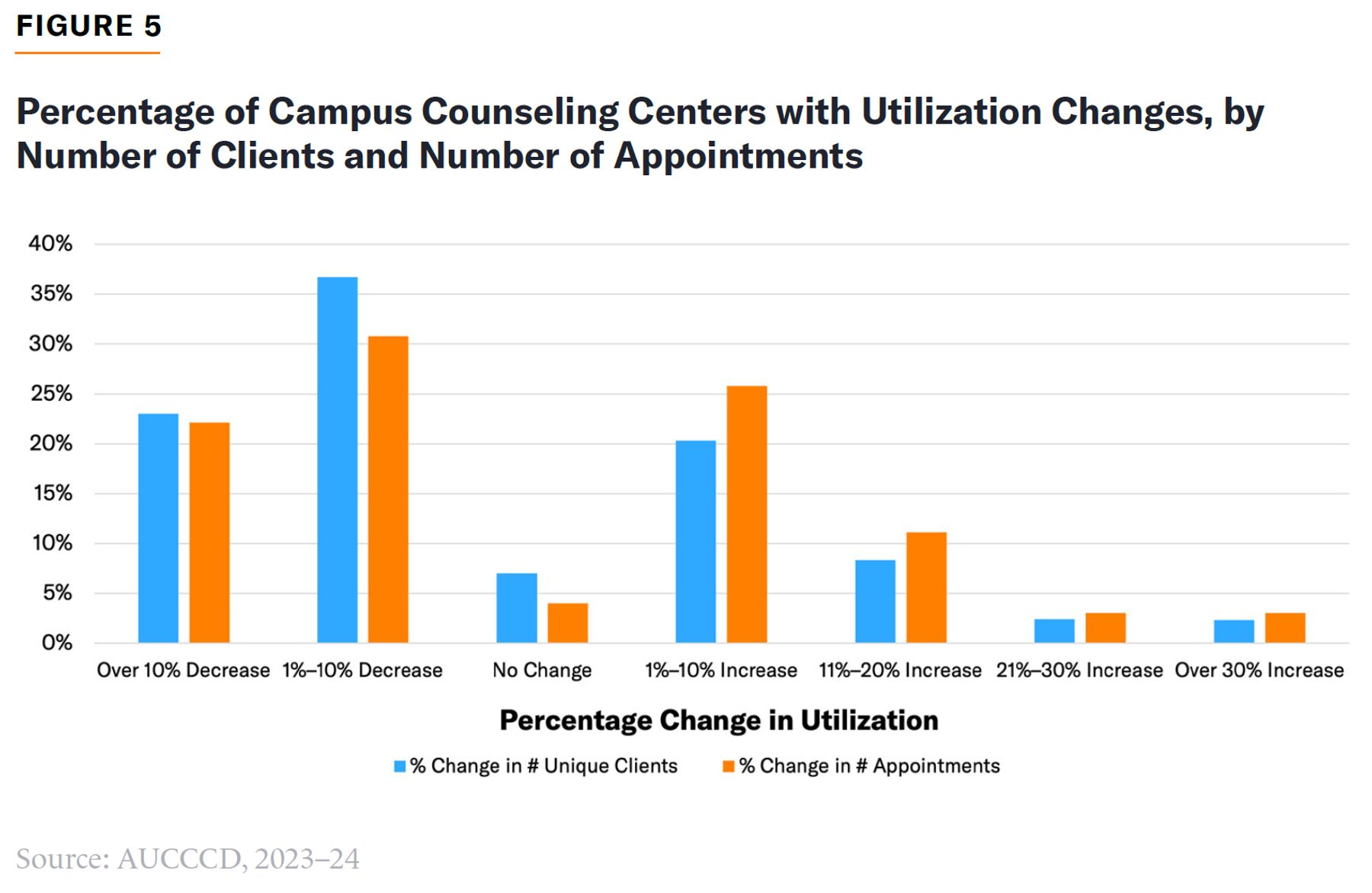
Despite claims of increased demand for campus mental health services (which have been made for decades),[79] a majority of AUCCCD respondents (61%) reported a utilization decline in 2023–24, compared with the previous year (Figure 5), with nearly 25% of centers at four-year institutions reporting a decline of over 10% in the number of clients served. Demand for mental health services can be subject to seasonality and economic effects[80] such as recessions,[81] so this decline may represent a pandemic-induced peak that is now subsiding. AUCCCD respondents may not be representative of all counseling centers, but take-up rates of counseling services, while they may vary cyclically, have not changed dramatically since their establishment. In 1948, caseload estimates of non-veteran groups served by counseling centers were between 3% and 11%[82]—almost exactly where they are today.
Broad mental health initiatives like awareness training have not reduced rates of mental health conditions: evidence shows that students need no training in order to recognize mental health problems and that many are already aware of available campus services. Depression is recognized at rates of nearly 90% in pretests for mental health awareness training.[83] National survey data show that student awareness of available services has consistently been above 50% since 2007, reaching nearly 80% in 2025.[84] Alarmingly, a growing number of academic researchers have raised concerns that mental health awareness efforts can worsen mental health outcomes and promote a sense of victimhood.[85] Treatment carries risks of iatrogenic harm when expanded indiscriminately.[86] Medications and therapies can have negative effects on symptoms and can cause symptoms to manifest.[87]
Overemphasizing mental health can direct students who do not have severe mental health conditions toward costly and more intensive medical services than are needed. Likewise, it can be harmful to frame all normal, mild, and moderate distress as appropriate for mental health services; doing so suggests that there is something wrong with emotional responses that are inherent to the human condition (which cannot be eradicated and can be adaptive).[88]
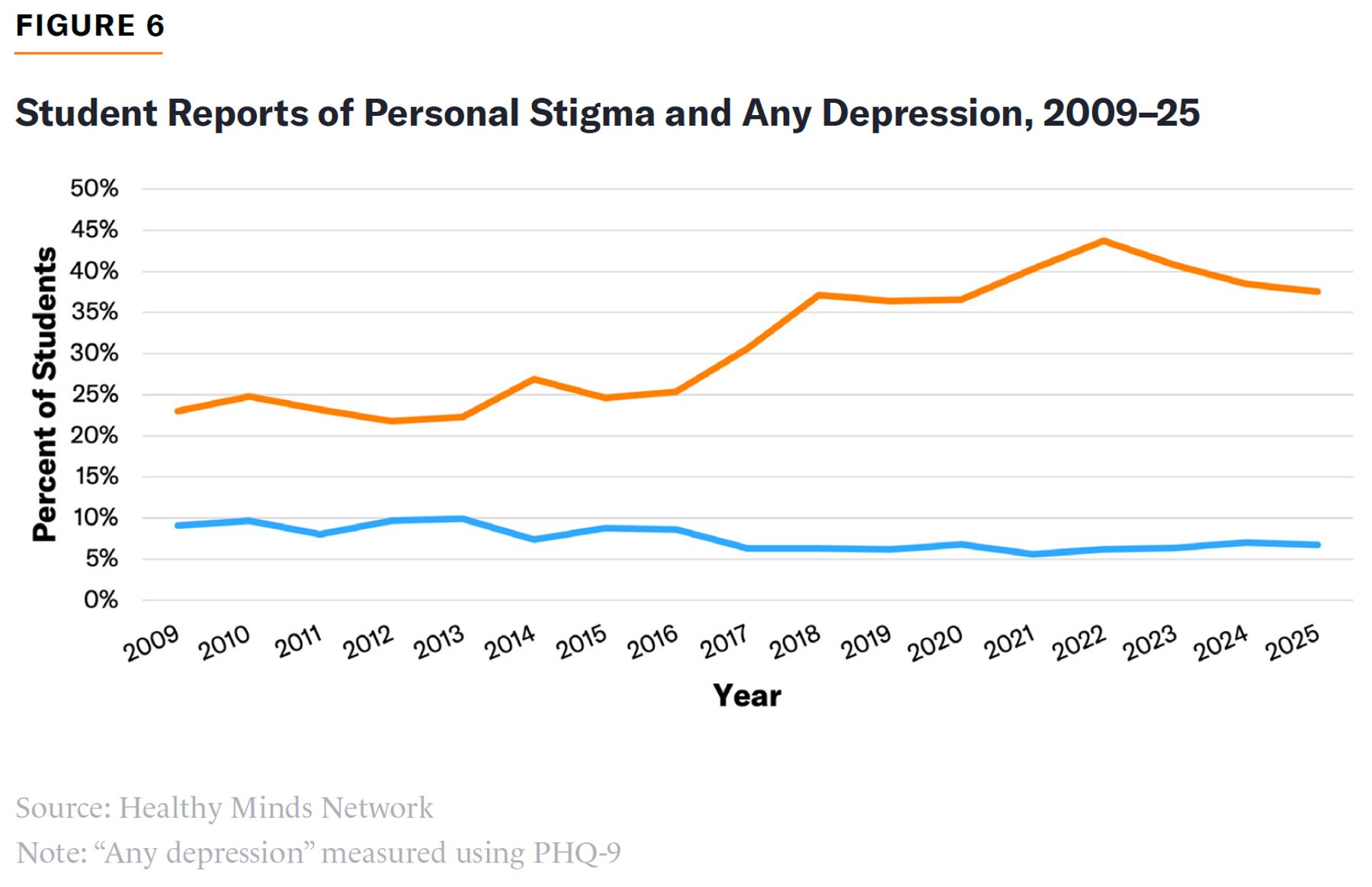
There is a downside to the normalization of mental health conditions. Destigmatization has been accompanied by a rise in reported distress. As shown in Figure 6, the decrease in the number of students who reported feeling stigma about seeking services (which was low to begin with) has corresponded with an increase in the number of students reporting depression symptoms.[89] Research has also found that stigma is not a deterrent of service utilization among college students of color.[90]
In recent years, as mental health conditions have been increasingly normalized—and the number of students reporting such conditions has grown—many schools have faced scandals related to students taking advantage of disability accommodations for benefits, as reported in the Wall Street Journal,[91] The Atlantic,[92] and other major publications.[93] In 2013, only 911 postsecondary institutions classified 3% or more of its student body as having disabilities; that number had increased to 1,675 by 2023,[94] an 83% rise. The percentage of undergraduate students with disabilities is highest at Ivy League universities (at least 15.5%) and lowest at public two-year institutions (6.1%).[95]
In a recent op-ed in the Times, “Nearly 40% of Stanford Undergraduates Claim They’re Disabled. I’m One of Them,” a Stanford student explained that many students were seeking accommodations as a way of getting nicer dorm rooms. But she explains that “almost no one” feels shame about doing so. “Rather, we openly discuss, strategize, and even joke about it. At a university of savvy optimizers, the feeling is that if you aren’t getting accommodations, you haven’t tried hard enough.”[96] The student admitted being willing to request housing for “legitimate illness—endometriosis” only because so many other students had received it for less severe ailments, such as ADHD,“night terrors,” or a simple description of “can’t live with others.”
The Conflict with Higher-Education Reform
Recent higher-education reform efforts have focused on increasing economic return on investment for students and taxpayers alike,[97] preparing students for productive participation in American society,[98] and facilitating higher learning and debate with an emphasis on ideological diversity.[99] Most campus mental health services do none of the above. Campus mental health, as currently conceptualized, is at odds with the goals of higher-education reform.
The cost of campus amenities has skyrocketed, and the cost of mental health and wellness services has been a concern among university presidents.[100] Colleges competing for a declining number of students must offer not only academic opportunities but amenities,[101] extensive dining options, and athletic facilities.[102] Wellness rooms with massage chairs fit squarely into this category. Such services drive up attendance costs and leave students in greater debt for no better academic offerings.
Young adulthood involves stressful life changes.[103] To the extent that IHEs seek to prepare students for the real world, encouraging students to view discomfort and unpleasant feelings as a problem for mental health providers or bureaucratic authorities is counterproductive—as are extra exam time and excused absences.
Mental health ideology can reduce students’ capacity for productive civic engagement. Medicalization can flatten community, as individuals turn to health and mental health professionals over other sources of support, such as family and faith. Excessive attention to one’s own mental state is self-focused, as opposed to selfless. This can reduce the obligation to “show up” for others—to use therapeutic terms—which is an important characteristic of dependable colleagues, neighbors, and citizens.
The “put your mental health first” ethos lowers academic accountability and expectations for students. Students now spend less time on academic work than in the past; yet they feel more stress about it, leading professors to reduce requirements.[104] Academic rigor is reduced while testing accommodations and comfort amenities, like relaxation rooms, become the norm.
It is often not recognized that mental health professions and programming are rooted in a fundamentally progressive ideology that involves psychological “safetyism,”[105] identity politics,[106] and social justice,[107] all of which can frustrate open debate and intellectual diversity.[108] Of course, not all individual mental health professionals are progressive radicals. Mental health professional associations, however, typically adopt explicitly ideological framings: the American Psychological Association, for example, promotes “equity, diversity, and infusion (EDI)” as essential in all aspects of its work,[109] as does the American Counseling Association, which also emphasizes social justice. When mental health services teach students that certain beliefs are “unsafe” or cause psychological harm, self-censorship is encouraged over evidence and respectful argument.
IHEs will not benefit by offering more of these services; in fact, allowing these services to become further entrenched risks fostering unrealistic expectations for what IHEs will provide students in terms of treatment options and for how students should expect to feel emotionally during a fundamentally transitional time of life. Expanding services also invites mission creep. Despite providing ample mental health services, colleges are still blamed by some as one culprit in the current “mental health crisis.” Consider a 2023 report by the educational consulting group College Futures Foundation, which argued that colleges are actively harming students’ mental health because they: (1) promote social isolation, especially for minority students; (2) sustain hostile climates for marginalized communities like LGBTQ+ students, undocumented students, and students of color; (3) promote individualistic, competitive attitudes; (4) uphold high costs and promote debt; and (5) create barriers to accessing mental health.[110]
None of these arguments can withstand scrutiny: First, colleges bring people together in a literal sense, whether physically or remotely. Second, few would argue that the environment on American campuses is one in which LGBTQ+, undocumented, and minority students are censured rather than celebrated. Third, extensive grade inflation since the 1990s undermines claims about excessive competition[111]—which, even if it were happening, should not be viewed as inherently problematic. As for high costs and debt, these are issues that reformers are concerned with. But these are questions of trade offs. For those of lower means, many colleges cap student tuition costs, and a college degree delivers a return on investment on average.[112] Debt represents available credit that allows far more students to access higher education than would be able to do so without it.
Finally, cost is also driven by offering services meant to attract students and improve their experience. If campuses are perceived as creating barriers to mental health access, despite substantial investments in mental health awareness, early intervention, screening, referral, diagnostic services, counseling and therapy, and even psychiatric services, then institutions should reconsider the benefit of such services.
Conclusion
IHEs should resist pressure to respond to every proclamation of a student mental health crisis with new programs or initiatives that do not further the goals of providing students with a rigorous education that prepares them for participation in a democratic society. IHEs should reevaluate their current mental health offerings and determine whether they are improving student outcomes, beyond superficial input measures such as the number of students served, absent any rigorous outcome metric. Schools should make clear to students that higher education will not necessarily be a stress-free experience but, rather, one that expects students to be able to overcome challenges. While IHEs must meet their legal obligations to serve students with disabilities, they should refrain from making those obligations more difficult to meet and inflating demand for accommodations by unnecessarily offering services that encourage students to seek treatment services, particularly if such services are not required or effective.
A disciplined approach to campus mental health requires first understanding what is currently being done on any given campus and determining the concrete ways in which any given service or programming is contributing to the institution’s vision of excellence and success. It is not enough to say that services should continue simply because they have long existed. Are services furthering the institutions mission? In what concrete ways? Particularly given obligations for students with disabilities, to leave these questions unanswered will inevitably facilitate reduced accountability—whether for students or the institution itself.
Institutions should also understand that campus mental health services are, in many cases, more akin to a student experience amenity than to health care. If treating mental health conditions is a goal of the institution, current programs that fall within or are related to mental health should be evaluated for their evidence of effectiveness to that purpose. If the primary mission of higher-education institutions is to provide high-value higher learning and facilitate a productive civil society, campus mental health programming should contribute to that mission. The open-ended mandate of “improving wellness” will do, and has done, little more than crowd out core responsibilities.
Acknowledgments
The author would like to thank Stephen Eide and Andy Smarick for their feedback.
Endnotes
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).