Mental Health First Aid Assessing the Evidence for a Public Health Approach to Mental Illness

Photo: PeopleImages/iStock
Since the 1960s, the prevailing strategy for addressing mental illness has not been treatment but a public health approach that devotes resources to education and prevention. This approach is manifest in Mental Health First Aid (MHFA)—an increasingly popular program originally implemented to prevent mental illness-related tragedies, theoretically by teaching everyday citizens “how to identify, understand, and respond to signs of mental illnesses and substance abuse disorders.”
The evidence that MHFA achieves this goal is lacking. Two decades of research show that it does not improve outcomes on relevant metrics, such as fewer crises or tragedies, reduced prevalence or disease burden of mental illness, or greater access to high-quality treatment and services.
- No studies demonstrate evidence that MHFA serves its purpose of helping individuals with mental illness in crisis, whether to connect them with treatment or improve their symptoms.
- Studies of MHFA largely measure success based on outcomes that are irrelevant to whether the targeted population benefits from the program.
- MHFA ignores the primary barriers to managing crises, such as scarce specialty health-care providers and services and insufficient treatment access for the mentally ill most at risk of crisis.
- Programs that aim to prevent mental illness should be met with skepticism, as the causes of mental illness are not fully known, and early intervention should target those most at risk.
Introduction
Lawmakers at all levels of government have promoted greater support for mental health policies in the wake of the Covid-19 pandemic, and typically do so following tragedies like the recent shootings in Buffalo, NY, and Uvalde, TX. President Biden’s 2022 State of the Union address[1] and FY 2022 Discretionary Budget Request[2] made commitments to health-insurance coverage and major investments to the mental health workforce. Governors in New York[3] and California[4] have recognized the inadequate infrastructure for psychiatric treatment and services, and NYC mayor Eric Adams has made addressing mental illness a critical aspect in improving public safety.[5]
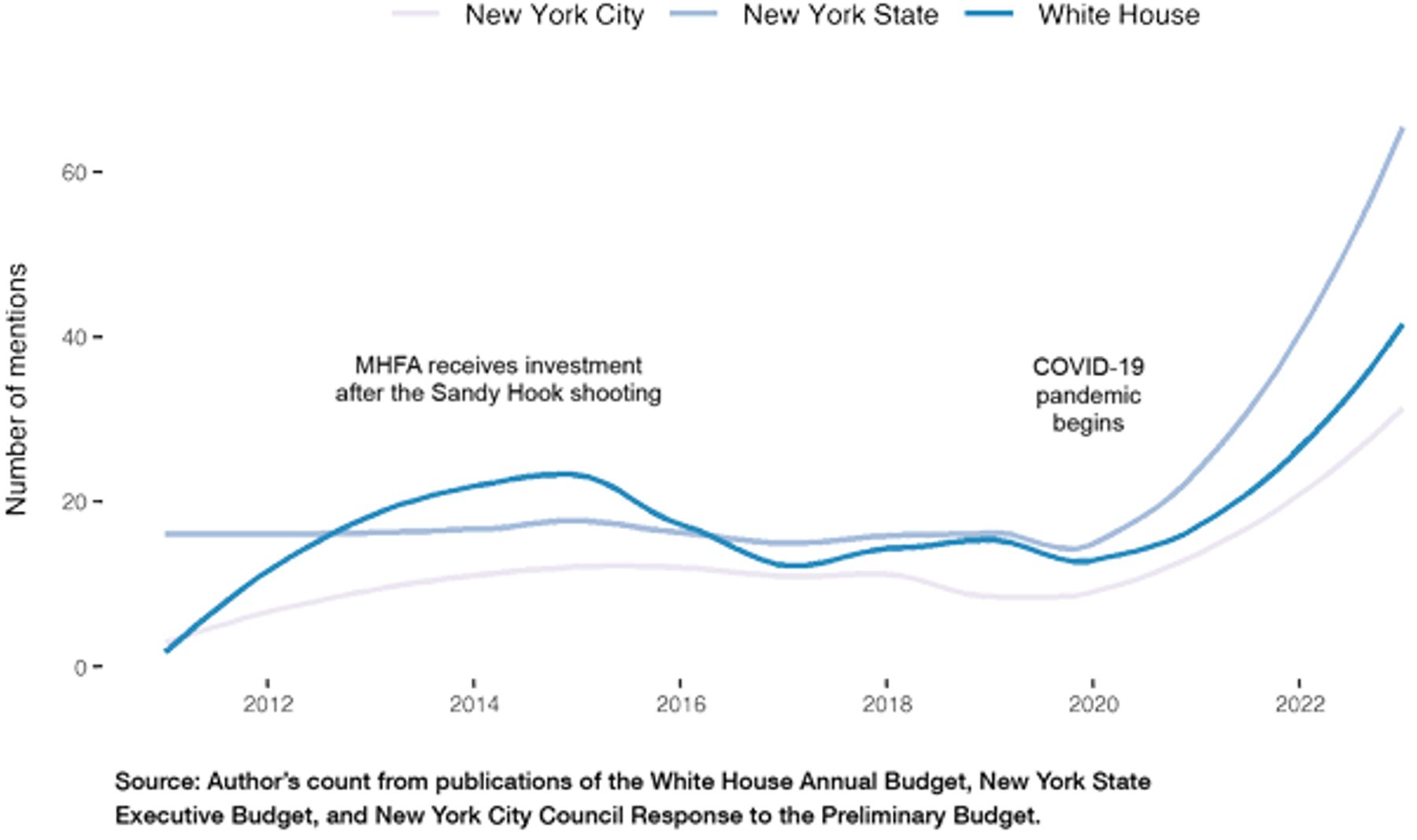
Figure 1
Mentions of “mental health” and “mental illness” in federal, state, and city budget documents (FY 2011–2023)
Treatment programs for serious mental illnesses, like schizophrenia or bipolar disorder, warrant government support, in part because there are market failures in the provision of health care and services for this population.[6] And, importantly, the consequences of untreated mental illness are borne by everyone in society, not just those who are afflicted.
Untreated mental illness leads to tragedies and reduced quality of life—for both the mentally ill and the public. In New York City, more than 13,000 homeless individuals are estimated to be severely mentally ill,[7] and untreated mentally ill individuals were involved in highly publicized subway attacks in 2021 and 2022.[8] Untreated mental illness is costly to taxpayers; the mentally ill disproportionately rely on Medicaid, Medicare, Social Security Disability Insurance (SSDI), and other public resources via the social service and justice systems.[9]
No single agency or level of government is wholly responsible for the treatment of mental illness.[10] One result of these compounded challenges is that many individuals go untreated.[11] Overall, fewer than half of people with a diagnosable mental illness receive treatment in a year.[12] Only about 16% of those with serious mental illness receive “minimally acceptable” treatment.[13]
Since the 1960s, the prevailing strategy for addressing mental illness has not been treatment but a public health approach that promotes education and prevention among the masses, in theory by focusing resources on social problems. This approach was inspired in part by perceived early success of military psychiatrists in treating soldiers with trauma outside hospital settings during World War II.
What Is Mental Health First Aid?
One example of a program taking a public health approach is the increasingly popular Mental Health First Aid (MHFA). MHFA is a commercially available course designed to teach everyday citizens “how to identify, understand, and respond to signs of mental illnesses and substance abuse disorders.”[14] In essence, it works similarly to that of a public screening program, meant to capture instances of disorder that otherwise may have gone unnoticed.
The overarching goal of the program is to connect mentally ill individuals—the intended beneficiaries—with an appropriate level of treatment before a crisis leads to tragedy. MHFA is premised on the idea of using education to create active bystanders: laypersons who can identify mental illness and are then willing and able to take action to provide help until professional treatment is received.
Over what’s typically an eight-hour training with instruction and role-play scenarios, MHFA teaches trainees about symptoms, prevalence, and risk factors of depression, anxiety, trauma, psychosis, and addiction disorders. According to the creators of MHFA, trainees learn an action plan to “approach the person [with mental illness], assess, and assist with any crisis; listen and communicate nonjudgmentally; give support and information; encourage the person to get appropriate professional help; and encourage other supports.”[15]
The nationally distributed MHFA product is managed and operated by the National Council for Mental Wellbeing (formerly the National Council for Behavioral Health) in partnership with the Missouri Department of Mental Health. These entities also offer a training product to certify instructors over a three-day course.[16]
MHFA first generated major interest after tragic, violent incidents involving untreated mentally ill individuals. In 2011, former congresswoman Gabrielle Giffords was shot in Tucson, Arizona by an individual diagnosed with paranoid schizophrenia.[17] Following the 2012 Sandy Hook Elementary School shooting by a young man not receiving treatment for psychiatric illnesses,[18] President Barack Obama subsequently proposed $15 million in funding for MHFA to train teachers in detecting and responding to mental illness in adolescents.[19]
In 2015, Congress passed the Mental Health First Aid Act, which provided $20 million for training more of the general public.[20] At least 20 states have separately funded MHFA since then. In FY 2022, MHFA-like programs were appropriated nearly $24 million, and the federal budget for FY 2023 increased that request to $64 million.
Figure 2
Substance Use and Mental Health Services Administration Budget Request, by Program Category (FY 2023)
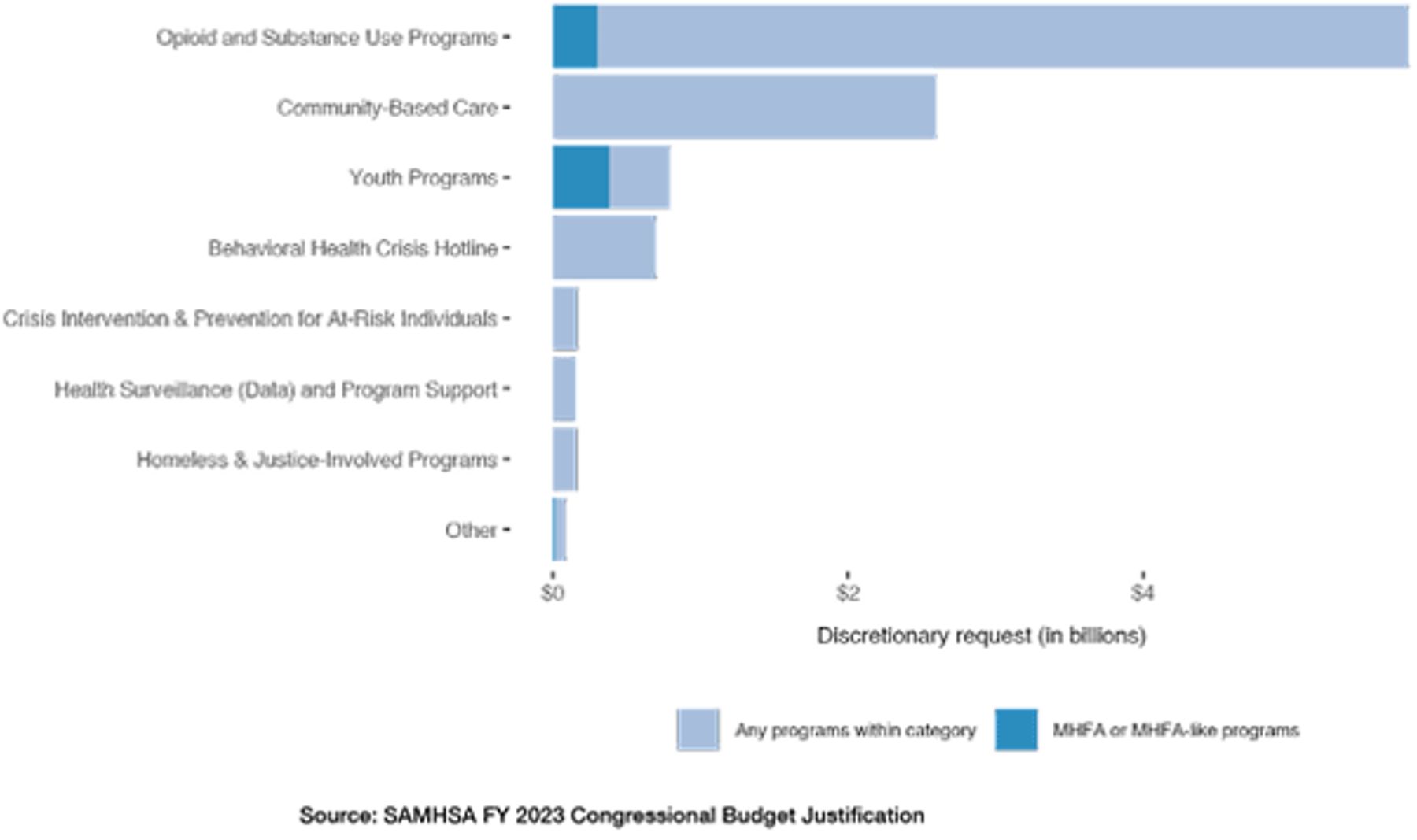
Spending on MHFA is small, in terms of the total spent annually on mental health at the federal level. But screenings and programs that take a similar preventative approach together receive significant public funding. MHFA is also increasingly being required of public agencies and schools at the state and local levels.[21]
Existing Evidence
Over two decades’ worth of evidence suggests that MHFA is ineffective. No studies reviewed demonstrate that MHFA succeeds in helping individuals with mental illness improve their mental health or receive appropriate treatment or services.
To examine the evidence base for MHFA, I identified publications via a Google Scholar search for “mental health first aid” and included all studies with a randomized control trial (RCT) design, all publications that specifically examined outcomes for the intended beneficiaries (which was uncommon) including meta-analyses, as well as any other publication with more than 50 citations. I also reviewed the 13 impact case studies promoted on the MHFA official website.[22] The result was 46 publications, 14 of which were RCTs, and only 7 of which examined MHFA’s effects on the intended beneficiaries. Notably, 16 publications were by an MHFA program creator, 14 of which had more than 50 citations (Table 1).
Table 1
Overview of MHFA Evidence Reviewed
| Total publications reviewed | 46 |
| Impact case studies from MHFA official site | 13 |
| Studies using a randomized control trial design | 14 |
| Publications examining a beneficiary outcome | 7 |
| Publications by an MHFA program creator | 16 |
| Studies showing that MHFA improves beneficiary outcomes | 0 |
| Note: All publications reviewed for this report can be found in Appendix A. | |
The most cited publication, with 471 Google Scholar citations, evaluates MHFA’s effect on knowledge of mental disorders, attitudes toward mental disorders, and trainees’ self-reported helping behavior (willingness to provide, or actually providing, MHFA to individuals).[23] The evaluation was published in 2002 by the MHFA creators. Trainees of a public course in Australia, where MHFA was created, were given a questionnaire to complete at the beginning of the first training session (a pre-test), at the end of the last session (a post-test), and six months after completion (follow-up).
At follow-up, trainees reported feeling more confident in their ability to help those in crisis but did not report actually providing help more often. The evaluation did not examine outcomes of intended beneficiaries of MHFA who received help from a trainee, such as whether more connections to treatment or services were made.
The study has several limitations, particularly in its design. A rigorous evaluation would randomly select individuals to participate, include a control group that does not receive MHFA training, and be conducted independently and free of any potential conflicts of interest. None of these aspects is present.
Without a random sample of participants in an evaluation, results cannot be generalized to the broader public. Individuals who proactively participate in MHFA could be inherently different from those who do not. Indeed, many trainees who participated were caregivers of mentally ill persons or health service providers, who could have stronger motivation to learn, and complete study questionnaires, than do others. Absent comparison with a randomly assigned control group that does not receive the training, outcomes cannot be attributed to MHFA; they could be an effect of some other program, event, or characteristic of the group.
Four studies of MHFA use an RCT, a rigorous evaluation method, and also specifically measure outcomes of recipients of help from a trainee. None found MHFA to be effective. A 2014 RCT evaluated MHFA as an approach to addressing access to mental health care for college students by training resident advisors (RAs) on several college campuses. Controlling for demographics, students in residence halls with RAs who had MHFA training were less likely to report receiving mental health support or treatment, as compared to those in a residence hall without MHFA-trained RAs. Even for residents who had an apparent baseline need for mental health treatment, service utilization did not increase after their RAs participated in MHFA.[24]
Many publications were not conducted independently and free of potential conflict of interest or possible bias; rather, they were authored by an MHFA program creator. Even so, none of them found evidence of any benefit for individuals with mental illness.
The MHFA official website highlights 13 case studies that purportedly show the program’s effectiveness.[25] The strongest evidence for support provided is weak. One case shares a trainee’s anecdotal story of persuading someone to “get the help he needs from his family and professionals.”[26] But it is not reported whether that individual sought treatment or was able to receive it. Another case attributes MHFA with the positive outcome of a viral story: a police officer successfully de-escalated an interaction with an individual with autism.[27] But the officer was asked by a CNN reporter whether his actions were a result of “training, or something you have just learned?" His response: "Just something that I have learned over the years."[28] No case studies on impact have been added to the MHFA official website after 2018.
Among all publications reviewed, spanning two decades, only in one was there evidence that MHFA had some type of effect that might affect potential beneficiaries. In an RCT of students whose teachers received MHFA training, students were more likely to report getting information about mental health problems, like a class lesson. But students were not more likely to have the teacher talk to them, listen, or suggest professional help—that is, the very type of intervention that MHFA trains teachers to give.[29] Students’ reported mental health was not improved by MHFA, even in a secondary analysis focusing just on those with worse mental health.
Neither of the organizations that manage and administer the national MHFA program provides a number of intended beneficiaries who have been connected to care per their individual public webpages, nor does the MHFA official website.
Irrelevant Outcome Measures
Figure 3
Most publications measure MHFA trainee outcomes rather than beneficiary outcomes
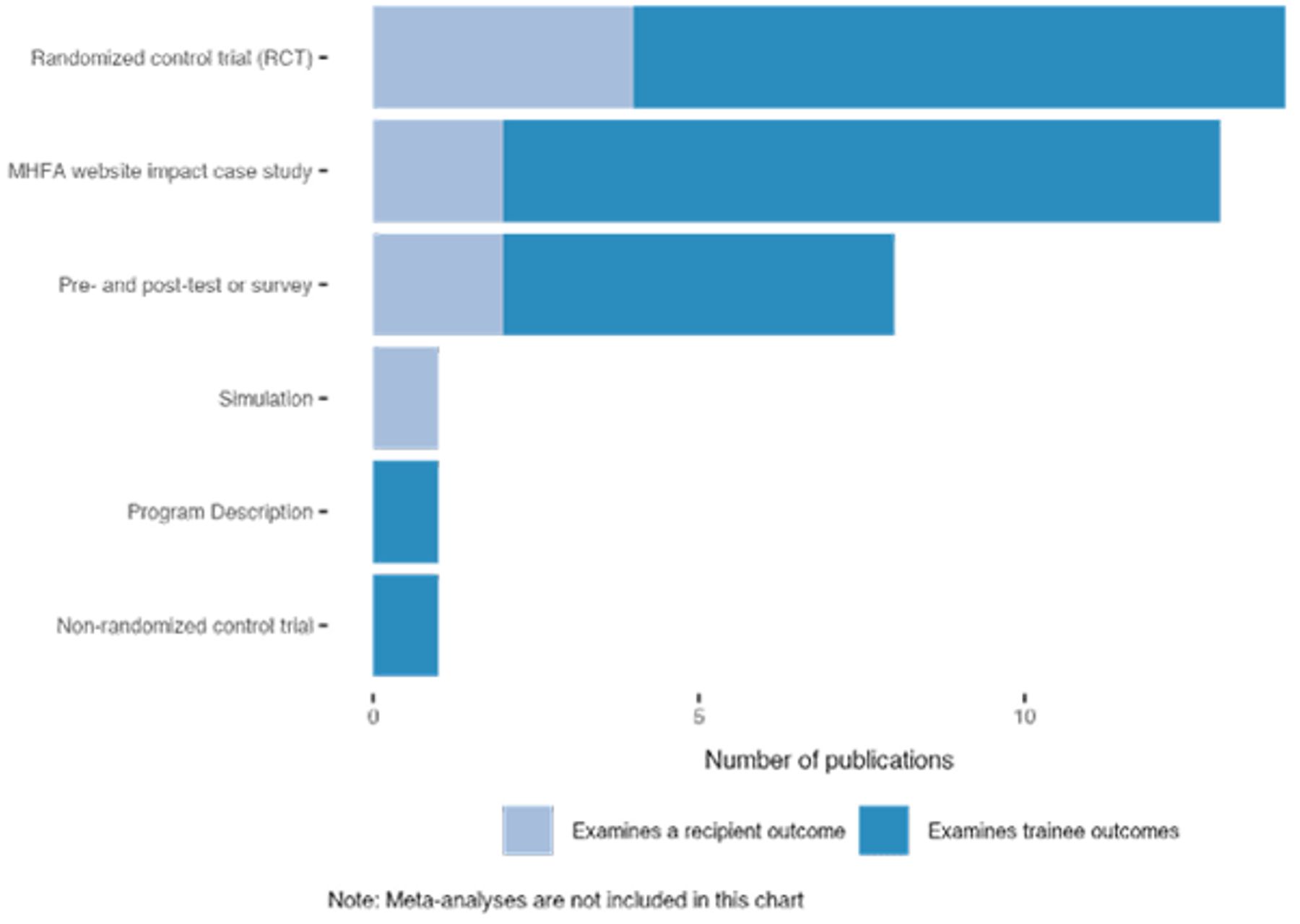
Most evaluations of MHFA focus on the outcomes of trainees or on entirely unrelated outcomes; few measure the program’s effectiveness in helping its intended beneficiaries—those with mental illness.[30] One meta-analysis finds that of 181 articles on MHFA, 90% focused on the educational benefits for trainees, and none focused on the effectiveness of patient help-seeking behavior.[31]
Two trainee benefits that are often promoted include self-reported confidence in ability to help and improved mental health literacy.[32] Research does not suggest that these outcomes translate into better outcomes for intended beneficiaries. In a 2019 RCT, trainees reported greater confidence and knowledge but did not provide better quality support to recipients, nor did recipients’ mental health improve.[33] Trainees also reported improved confidence in a 2018 study, but when simulated situations with depressed and suicidal patients were observed, trainees did not apply what they supposedly learned. In one particularly silly framing of supposed useful knowledge gain, a study by the program’s creators claims merit because Mental Health First Aid “appears to be an effective and feasible program for training … Mental Health First Aid.”[34]
MHFA subscribes to the notion that help is not sought or received in part because individuals with mental illness are stigmatized, so many evaluations examine whether trainees’ attitudes toward mental illness change as a result of the program. One publication assesses this argument well: “Considerable progress has been achieved in improving public awareness of mental illness and reducing its stigma. However, this has not driven substantial changes in access to and quality of mental healthcare.”[35]
An unrelated outcome often used as supportive evidence for MHFA is the number of individuals trained. This is the primary metric for all 13 case studies on the official site, which also offers that “more than 2 million” people are MHFA-trained in the United States.[36] But this measure does not indicate effectiveness, and as the program is ineffective, then training more people is not a benefit.
Potential Unintended Consequences of MHFA
MHFA trainees may feel ready or obligated to step in, inappropriately, during a dangerous crisis scenario where greater professional support is needed. While most individuals with mental illness are not violent, a small number of those with untreated serious mental illness are at higher risk of violence—this was precisely the case for the individuals who inspired the program’s federal support.[37]
MHFA may also change the help-seeking behavior of trainees and result in overdiagnosis. In the 2014 RCT of MHFA on colleges campuses, RAs were more likely to seek professional help themselves. In another study, individuals who did not report experiencing a mental health problem before MHFA training afterward reported that they were. This did not occur for the control group, and the result was statistically significant.[38] “Over-diagnosis of life problems as mental disorders,” as the authors describe, leads to overtreatment that is not beneficial, could cause harm, generates costs, and diverts resources from the most severely ill.[39]
The Flawed Underlying Approach
MHFA is representative of a public health approach that prioritizes education and prevention among the masses over treatment of current cases of mental illness. This approach has failed to improve important outcomes. Rates of mental illness in the U.S. have not decreased.[40] Rates of suicide have increased.[41] Mentally ill individuals persistently experience lower life expectancy,[42] are disproportionately represented in homeless and incarcerated populations,[43] and are the subject of hundreds of thousands of 911 calls annually.[44]
Recognizing Mental Illness Before Tragedy
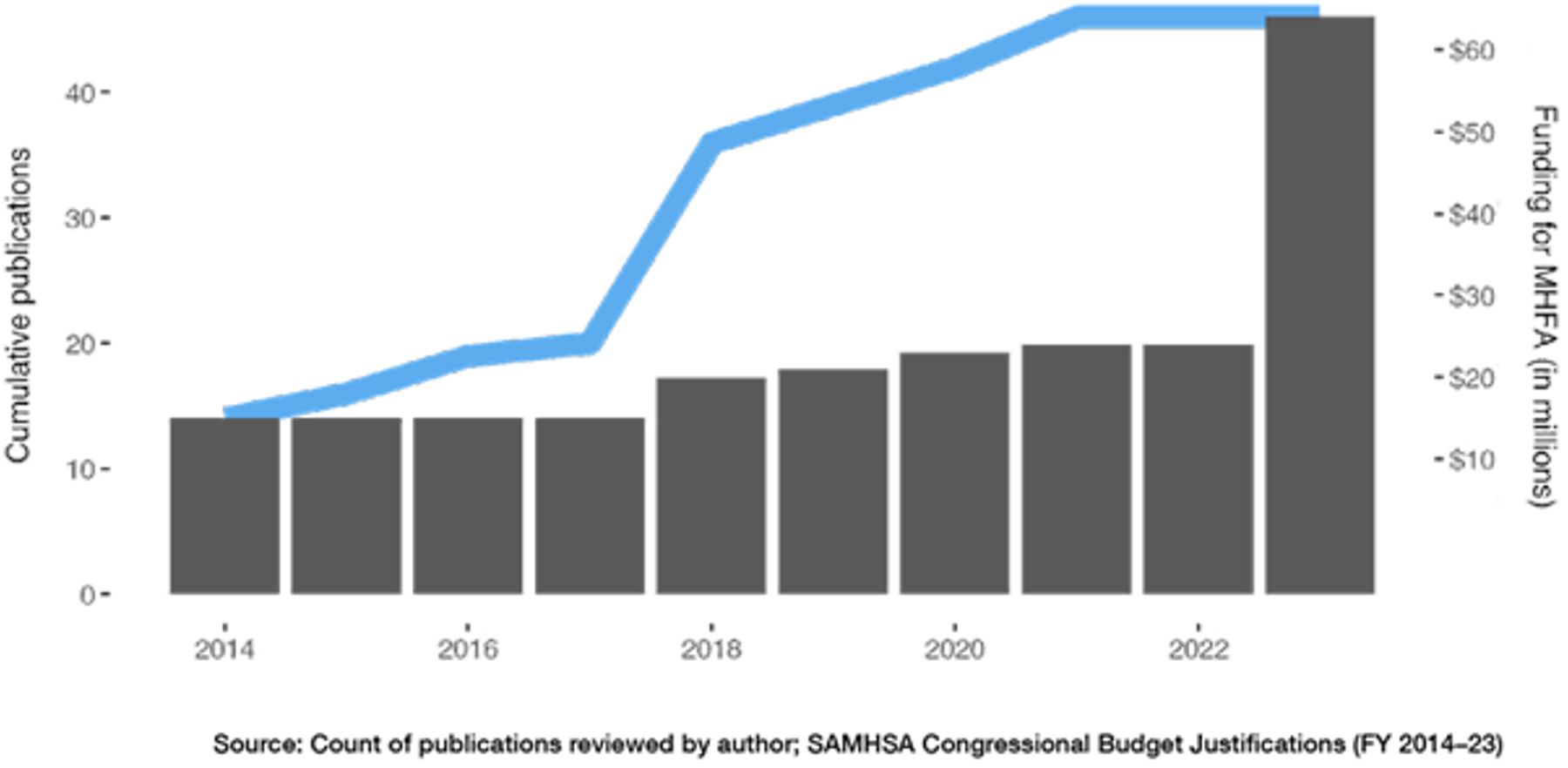
Figure 4
Despite cumulative evidence that MHFA is not effective (blue line), federal funding for the program continues to increase (gray bars)
The underlying premise of MHFA is that a lack of knowledge about mental health leads mental illness to go unrecognized, which means people are not connected to treatment and fewer crisis situations are averted. This theory is akin to that of a public screening program meant to capture disorders that might otherwise go unrecognized absent a screening. But lack of recognition is not a demonstrated problem. In multiple studies, MHFA trainees overwhelmingly recognized mental illness—even symptoms of specific diagnoses—prior to the training,[45] in representative cases, recognizing depression 89.6% of the time[46] and schizophrenia 81.7% of the time.[47] Families of severely mentally ill individuals often desperately seek—and cannot attain—intervention for their loved ones whom they know are sick and in crisis. Those family members can end up victims of violence,[48] not for lack of knowledge or recognition.
The mentally ill individuals responsible for the tragedies inspiring federal funding of MHFA were known to have psychiatric disorders.[49] The same was true of the Parkland shooting in 2018.[50] Media reports of mental illness-related tragedies regularly quote family members who say their relation was diagnosed mentally ill but not treated,[51] had been in and out of treatment,[52] or was released from hospitalization too soon or without follow-up.[53]
MHFA tries to prevent tragedies by casting the widest net possible, identifying every case of mental illness or emotional distress—however minor, asymptomatic, or at risk of crisis. The tragic shootings in May 2022 in Buffalo, NY, and Uvalde, TX, made clear, however, that the resources available are not abundant enough to manage even all known individuals who explicitly assert intentions to act violently, or who act erratically enough to warrant early intervention and monitoring. To dilute the pool of in-need individuals with false positives further restricts opportunity to effectively allocate professional help.
Preventing Mental Illness “Upstream”
MHFA gets the timing wrong: when tragedies from mental illness occur, it’s not usually a surprise and—unlike traditional First Aid—it could likely be too late for a layperson to safely or effectively intervene.
MHFA and other upstream intervention do not prevent mental illness from developing or reverse its effects. Preventing mental illness is contingent on understanding its causes. But, as the MHFA manual admits, those causes are unknown.[54] Even in secondary prevention—detecting disease in early stages—mental illness faces challenges;[55] there are no single biomarkers,[56] lab tests,[57] or imaging tools[58] for confirming mental illness, and being at risk does not mean mental illness will manifest with certainty.[59]
Mental illness manifests out of a combination of genetic factors, exposure to environmental stressors before birth (like inflammatory conditions or toxins), and impaired brain chemistry.[60] Offspring of parents with serious mental illness are at high risk of developing psychiatric disorders by early adulthood.[61] Physical health problems have also been causally associated with developing depression and anxiety.[62] Certain social circumstances may increase the risk of developing some mental illnesses.[63] PTSD, for example, can occur from exposure to death, sexual violence, or the threat of either.[64]
Mental illness can’t yet be prevented. But absent accountability for programs to demonstrate evidence of success on relevant beneficiary outcomes, in high-quality evaluation, “preventing mental illness” becomes an excuse to dole out public dollars to any given concern of the day—like poor grades or job loss—by claiming that it could improve reactions to negative life situations. In his 2022 State of the Union mental health strategy, for example, President Biden suggests mental health funding be used to stop “discriminatory algorithmic decision-making that limits opportunities for young Americans”—such as when a girl (as opposed to a boy) searches for jobs online and is not immediately shown fields for engineering—because when “people are treated unfairly, it can have mental health impacts.”[65]
To be clear, mitigating social and economic problems is a worthy policy goal, but almost none of the individuals who experience one of these common adverse life events will go on to develop a psychiatric disorder that leaves them gravely disabled or leads them into crises like violence, incarceration, or homelessness. The prevalence rate of schizophrenia is incredibly low, with estimates typically below 2%.[66] And the prevalence of any serious mental illness is estimated to be around only 5%.[67] If mental health spending is not directed primarily toward those with serious mental illness, at risk of crisis from mental illness, and in need of treatment for mental illness, these individuals will receive public support to a lesser extent than others who may receive support through programs delivered by non–mental health agencies.
Treating Mental Illness Should Be Prioritized
Treating current cases of mental illness is deprioritized by a public health approach aimed at education and prevention.[68] Perhaps unsurprisingly, MHFA ignores primary barriers to managing mental illness-related crises: treatment access for the mentally ill most at risk of crisis and a scarcity of specialty health-care providers and services. These issues are widely acknowledged in academic and policy literature.[69]
A case study on the MHFA website notes a “worrying statistic” that in Jacksonville, Florida, “it takes 14–30 days to get access to mental health resources”[70] but faults stigma associated with seeking treatment, not a lack of resources themselves. MHFA trainees who don’t stigmatize mentally ill persons will still be ineffective when there are no services to offer.
More than half of all U.S. counties have no actively practicing psychiatrist, and more than two-thirds have no actively practicing child and adolescent psychiatrist.[71] Psychiatrists are also highly concentrated in the northeastern United States and California. Rural counties have a significantly lower portion of psychiatrists than do metropolitan areas.
Physical infrastructure for treating mental illness is inadequate. There is a national shortage of psychiatric beds,[72] driven by payment structures that disincentivize providers from offering inpatient treatment. Medicaid largely discriminates against coverage of services for mentally ill individuals treated in specialty psychiatric hospitals with more than 16 beds (called Institutions for Mental Disease, or IMDs),[73] and psychiatric care in general hospitals is also offered sparsely, as psychiatric services are much less profitable than other services a hospital can choose to offer, like cardiovascular surgery, neurosurgery, and gastroenterology.[74]
Where services are available, individuals most at risk of crisis or tragedy—those with serious mental illnesses—are least likely to be accepted by providers if they do seek treatment.[75] Their cases are the most complex, can be difficult to manage, and are poorly reimbursed. Many mentally ill are uninsured or insured by Medicaid, but more than 60% of psychiatrists do not accept Medicaid; 43% of psychiatrists in private practice are less likely to accept any insurance at all.[76] Despite federal requirements of hospitals participating in Medicare to accept patients into emergency departments regardless of insurance status, violations against psychiatric patients are common—seriously mentally ill individuals are turned away from hospitals,[77] not accepted into specialty hospitals, and are often released without being stabilized.[78]
Recommendations
Programs that receive public mental health funding should be assessed for and demonstrate effectiveness using meaningful outcome measures. Examples might include greater access to high-quality treatment, engagement and continuation with treatment, reduced disability from serious mental illness, symptom management, and fewer incidences of violence, homelessness, and incarceration among the mentally ill. Process measures unrelated to outcomes of intended beneficiaries—like the number of program participants or participants’ satisfaction with a program—are not evidence of value-add and do not alone warrant program support.
Two programs with strong evidence of success on meaningful outcomes are Assisted Outpatient Treatment (AOT) and Assertive Community Treatment (ACT). AOT is a form of intensive community-based treatment and care-coordinating services accessed through civil court and meant for mentally ill individuals who meet strict criteria such as repeated episodes of hospitalization, arrest, and incarceration. It is implemented on the state and local levels but can also receive federal funding. Research on New York State’s AOT law (Kendra’s Law) has found that it helps individuals stay in treatment[79] and that fewer participating individuals engaged in harmful behaviors to self and others, or experienced arrest, incarceration, homelessness, and hospitalization.[80]
ACT is a similar effective approach for individuals with severe mental illnesses. A multidisciplinary team works together to provide a comprehensive set services like community-based treatment, case management, and employment support. SAMHSA reports that teams find they can anticipate and avoid crises.[81] A Rochester, NY, adaptation meant to reduce recidivism and promote recovery among justice-involved adults with a serious mental illness found it to be associated with fewer convictions for new crimes, less time in jails and hospitals, and more time in outpatient treatment.[82]
Other worthy programs include mental health courts, which operate similarly to AOT but through the criminal court system, and have demonstrated success in reducing recidivism and violence.[83] Supportive housing reserved for mentally ill individuals (for whom it was originally designed) offers services like case management alongside subsidized housing and has significant cost savings to government on other services for the homeless mentally ill.[84]
Treating present cases of serious mental illness should be a central policy goal. Intensive community treatment focused on individuals with serious mental illness is so minimally prioritized that leveraging the legal system (as AOT and mental health courts do) has become the mechanism by which the most are able to access what they would have difficulty accessing otherwise[85] because more mild or moderate cases are more likely to be served.
Investment in essential infrastructure, like inpatient bed capacity, could help meet treatment needs by expanding available services and providing greater opportunity for access. Inpatient psychiatric hospitals, by their very nature, serve individuals whose mental illnesses are most debilitating, and general hospital psychiatric units play an important role in treating medically complex mentally ill patients in crisis. Many financial incentives exist in insurance and payment systems that compel providers to avoid mentally ill patients and discourage maintaining appropriate capacity.
Because mental illnesses cannot be prevented without knowing their cause, prevention programs should be met with skepticism. Early intervention programs should be focused on those at highest risk of developing mental illness.
Appendix A
Table 1
All studies reviewed and the outcomes that each study measured
Table 2
Common evaluation measures of MHFA, described
| Recognizing mental illnesses | Trainees evaluated after MHFA might be shown vignettes of specific illnesses by their symptoms and asked to identify the illness. |
| Knowledge of mental health / MHFA | Trainees might be asked questions about content taught in the MHFA course to show whether they retained information they learned through the training—sometimes referred to as mental health literacy in publications. Questions might be about specific illnesses or the MHFA approach (e.g., “If someone has a traumatic experience, it is best to make them talk about it as soon as possible”). |
| Beliefs about appropriate treatment | Trainees might be evaluated on whether their beliefs are in concordance with professionals about appropriate types of treatment or help that could benefit a person with mental health problems (e.g., professional medical help), and whether they would be appropriate for a person in mental health crisis to speak with (e.g., family member, priest, counselor, general practitioner). |
| Confidence in ability to help / intention to help | Trainees are asked if they feel confident that they could help a person in mental health crisis by providing Mental Health First Aid, and/or self-report their intent to help in a hypothetical situation involving a person who might need help. |
| Actual helping or supportive behavior | Trainees are asked if they provided help or support to a person whom they thought might have a mental health problem. |
| Quality of helping or supportive behavior | The quality of trainees’ helping behavior might be rated, such as on a scale, based on whether they provided the specific types of help taught by MHFA (assess and assist with any crisis; listen nonjudgmentally; give support and information; encourage appropriate professional help; encourage other supports). |
| “Stigmatizing” attitudes | Trainees might report their own beliefs and perceive beliefs of others about whether mentally ill persons were dangerous, weak, unpredictable, and/or dependent. Vignette statements could be provided for participants to rank, e.g., “People with a mental health problem could snap out of it,” “John’s problem is not a real medical illness,” “People with a problem like John’s are dangerous,” “People with a problem like John’s are unpredictable,” “A problem like John’s is a sign of personal weakness,” and “It is best to avoid people with a problem like John’s.” |
| Social distance | Trainees self-report how willing they are to have contact or interpersonal relationships with a person described in vignettes of mental illnesses (e.g., being a neighbor, spending a weekend with, being a friend, being a workmate, or marrying into family). |
| Other trainee behaviors | Trainees might report that they feel better about taking the training if they perceive their own mental health differently, if they were satisfied with the training, or if they themselves seek help. |
Acknowledgments
The author would like to acknowledge Kaitlin Edwards for substantive research assistance and editorial contribution. The author would like to thank Jodi F. Paroff, Mabel Fung, Stephen Eide, and Daniela Moreira for valuable feedback. The author would like to recognize the late DJ Jaffe, as well as those he championed, as a primary source of inspiration.
About the Author
Carolyn D. Gorman is an adjunct fellow at the Manhattan Institute, where her research examines how policy changes in the U.S. health and judicial systems affect individuals with serious mental illness. She served on the board of the former Mental Illness Policy Org., a nonprofit founded by the late DJ Jaffe, and as staff on the U.S. Senate Committee on Health, Education, Labor and Pensions. Previously, Gorman was the senior project manager for mental illness policy at Manhattan Institute and has held research and policy positions in the private and nonprofit sectors. Her writing has appeared in the Wall Street Journal, New York Daily News, New York Post, City Journal, National Review, The Hill, and the peer-reviewed Psychiatric Services. Gorman holds a B.A. from Binghamton University and an M.S. in public policy from the Robert F. Wagner Graduate School of Public Service at New York University.
Endnotes
Photo: PeopleImages/iStock
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).