U.S. Psychiatric Hospitals Under Medicaid’s Institutions for Mental Diseases (IMD) Exclusion

Photo: Luis Alvarez / DigitalVision via Getty Images
Executive Summary
Many Americans with serious mental illness lack access to inpatient psychiatric care. For decades, Medicaid’s “institutions for mental diseases” (IMD) exclusion has been a major barrier to expanding psychiatric hospital bed capacity, but the ongoing mental-health crisis has recently led policymakers to consider repealing or modifying the IMD exclusion.
This report analyzes the size, ownership, and percentage of Medicaid discharges from freestanding U.S. psychiatric hospitals to show that to meaningfully increase Medicaid beneficiaries’ access to care in this setting, the IMD exclusion should be either completely repealed or significantly reformed.
Key findings include:
- The average size of a U.S. psychiatric hospital is 108 beds—smaller than the average general hospital—and 95% of all psychiatric hospitals are under 305 beds. Perceptions of psychiatric hospitals as very large-scale institutions are therefore misrepresentative.
- Less than 8% of psychiatric hospitals have 16 beds or fewer, the limit for federal financial participation. The vast majority of psychiatric hospitals are therefore not covered settings for Medicaid beneficiaries under the IMD exclusion.
- Since its establishment in 1965, the IMD exclusion has been repeatedly modified. Yet changes have not increased beneficiaries’ access to psychiatric hospital treatment at scale. The number of public psychiatric beds, which are most likely to serve Medicaid patients, is down by over 97% since its peak and remains low despite a decade of exemptions that allow greater Medicaid coverage.
- Analysis of hospital data and prior reforms suggests that further modest modifications of the IMD exclusion will not suffice to increase bed supply. Full repeal would be ideal, but if that’s not politically feasible, IMDs should, at a minimum, be defined as facilities with more than 108 beds (up from the current 16 beds). This would allow as many as 332 existing psychiatric hospitals (with more than 20,000 beds) to receive Medicaid reimbursement for their services.
Introduction
Medicaid is an important publicly funded health-care program for many of the 14.6 million U.S. adults with serious mental illnesses.[1] Among non-elderly adult Medicaid enrollees, 10% have a serious mental illness.[2] Medicaid enrollees are 90% more likely to a have a serious mental illness than privately insured Americans.[3]
Those with serious mental illnesses sometimes require inpatient care at specialty hospitals to meet clinical and safety needs.[4] However, the U.S. faces a shortage of psychiatric inpatient beds.[5] The number of public beds, in particular, has declined by over 97% since peak levels in 1955, accounting for population change.[6]
The bed shortage was first catalyzed, and has since been maintained, by a 1965 statutory provision known as the “institutions for mental diseases” (IMD) exclusion, which bars Medicaid from paying federal matching funds for psychiatric hospital treatment. The IMD exclusion—which mirrored preexisting rules excluding persons with psychosis from Social Security old-age assistance[7]—was intended to prevent states from shifting to the federal government the cost of mental-health-care treatment, which in the 1960s was almost entirely provided by state asylums.[8]
The Medicaid program defines an “institution for mental disease” as “a hospital, nursing facility, or other institution of more than 16 beds, that is primarily engaged in providing diagnosis, treatment, or care of persons with mental diseases, including medical attention, nursing care, and related services.”[9] Generally, the “overall character” of a facility is how the federal government assesses whether a facility is an IMD.[10]
Outside Medicaid, the term “IMD” has no meaning. IMDs are not a specific provider type recognized by insurers, state licensure agencies, or accrediting bodies.[11] IMDs are regulated under a variety of federal and state rules, but generally, facilities licensed or accredited as psychiatric hospitals are considered IMDs. Residential treatment facilities that treat both mental-health and substance-abuse disorders—often a step down from more intensive hospital care—are also typically considered IMDs.
The IMD exclusion prevents such facilities from providing mental-health care to Medicaid beneficiaries by banning federal financial participation (FFP)[12] to such providers for services rendered. States can elect to cover IMD services under Medicaid, but the state is responsible for the full cost of that care—unlike in virtually all other settings, in which the federal government covers at least half (and as much as 83%[13]) of the cost.
Perhaps the clearest sign of the shortage of psychiatric beds is that in nearly every state, there is a waiting list for such beds for forensic patients (those who receive psychiatric treatment as a result of being charged with or convicted of criminal behavior, typically to evaluate or restore competency to stand trial, or if found not guilty by reason of insanity).[14] As the number of state hospital beds has hit historic lows, a majority of them are now occupied by forensic patients, leaving few beds available for civil patients who need hospital-level psychiatric care.
The total number of forensic patients in state hospitals increased by 76% between 1999 and 2014, increasing from about 13,394 patients on a given day to more than 23,574 (in 37 states reporting), even as the overall number of psychiatric beds fell.[15] Inmates across 26 states wait a median of 60 days for a bed for competency restoration, according to research by the Treatment Advocacy Center, and at least 12 states have been sued for failing to provide timely competency restoration.[16]
The shortage of inpatient psychiatric care is evident in several other ways: high rates of mental illness among the homeless[17] and incarcerated;[18] greater average utilization rates in psychiatric inpatient settings compared with other health-care inpatient settings;[19] and the widespread practice of boarding mentally ill patients in emergency departments (EDs).[20] This last issue is especially costly, but without sufficient psychiatric beds, mentally ill individuals end up in EDs more often and for longer than nonpsychiatric patients. Psychiatric patients wait up to three times as long for a transfer from an ED to an inpatient unit, compared with patients with other conditions.[21] Of people with at least 18 ED visits per year in San Francisco, 87% had a mental illness or substance-use disorder.[22]
The lack of psychiatric beds—along with a continued recognition of the importance of inpatient treatment in the full continuum of mental-health care—has led Congress to limit the IMD exclusion in various ways.[23] But in recent years, amid a worsening mental-health crisis, support for more wholesale change has been growing:[24] the 118th Congress saw the introduction of legislation that would either fully repeal the IMD exclusion[25] or change the definition of an IMD to allow FFP at facilities with 36 or fewer beds, up from 16 beds.[26]
Current Landscape of Psychiatric Hospitals
To understand how repealing or reforming the IMD exclusion would help expand access to psychiatric care, it is first important to understand the supply of existing freestanding psychiatric hospitals, which are distinct from psychiatric units in general hospitals (which are not considered IMDs).[27] Psychiatric hospitals tend to offer more specialty mental-health services and more robust programming, such as youth-specific services.[28] Psychiatric hospitals can also provide services at lower costs than general hospital psychiatric units.[29] Further, some patients can be served appropriately only in psychiatric hospitals, as opposed to general hospital psychiatric units, because psychiatric hospitals—especially public psychiatric hospitals—are equipped to care for those who may become violent.[30]
Even though they are not subject to the IMD exclusion, general hospitals have also been cutting back on inpatient psychiatric services: federal survey data show that 612 general hospitals had 24-hour inpatient psychiatric units in 2022, down from 1,290 in 2012.[31] For general hospitals, psychiatric services are less lucrative than nearly all other services. Research finds that fewer than one in four general hospitals report having inpatient psychiatric beds.[32] Absent significant increases in reimbursement rates for psychiatric services, general hospital psychiatric beds are always at risk of being repurposed for more profitable uses.[33] This speaks to the importance of freestanding psychiatric hospitals’ role in providing inpatient mental-health care.
The data most commonly used to estimate inpatient psychiatric bed capacity come from the National Mental Health Services Survey (N-MHSS)—as of 2021, it’s called the National Substance Use and Mental Health Services Survey (N-SUMHHS)[34] —which provides an annual census of behavioral-health treatment facilities in the United States.[35] While the survey includes some information about facility characteristics, it does not report bed counts per hospital.[36]
An alternative source, the Centers for Medicare and Medicaid Services (CMS) Hospital Provider Cost Report offers more granular data on U.S. psychiatric hospitals, including specific bed counts per hospital and other details such as ownership. This granularity provides greater insight into the effect of the IMD exclusion’s 16-bed threshold on hospitals. Table 1 shows summary statistics for psychiatric hospitals in the 2022 CMS data.
Table 1
Summary Statistics of Freestanding Psychiatric Hospitals, by Ownership
| Group | Hospitals | Beds | Mean No. of Beds | STD | Min | 25% | 50% | 75% | Max |
| All | 580 | 62,439 | 108 | 93 | 3 | 48 | 88 | 130 | 639 |
| For-Profit | 352 | 31,693 | 90 | 52 | 12 | 49 | 86 | 119 | 315 |
| Public | 156 | 24,921 | 160 | 140 | 14 | 56 | 110 | 232 | 639 |
| Nonprofit | 72 | 5,825 | 81 | 72 | 3 | 16 | 65 | 113 | 335 |
Most psychiatric hospitals are small to midsize, with an average of 108 beds and a median of 88 beds.[37]
It is worth noting that the average psychiatric hospital has fewer beds than the average short-term acute-care hospital (i.e., general hospital), as well as the average children’s hospital, Veterans Affairs hospital, and Department of Defense hospital.[38] Perceptions of psychiatric hospitals as very large-scale institutions are therefore misrepresentative, and these hospitals exist, on average, on the smaller side of other hospital types, including general hospitals where FFP is not barred for care in psychiatric units.
Although not shown in the table, just under 8% of psychiatric hospitals have 16 beds or fewer, accounting for 1% of all beds. Ninety-five percent of all psychiatric hospitals have fewer than 305 beds, although the largest 5% of hospitals account for 19% of total beds. There are 29 hospitals with over 305 beds, and 26 of them are public hospitals that serve forensic patients.
Nearly 61% of psychiatric hospitals are for-profit; 27% are public (primarily state-run). Note, however, that although this report groups hospitals by ownership type, any discussion about the differences in the quality of care between ownership types is outside the scope of this report.
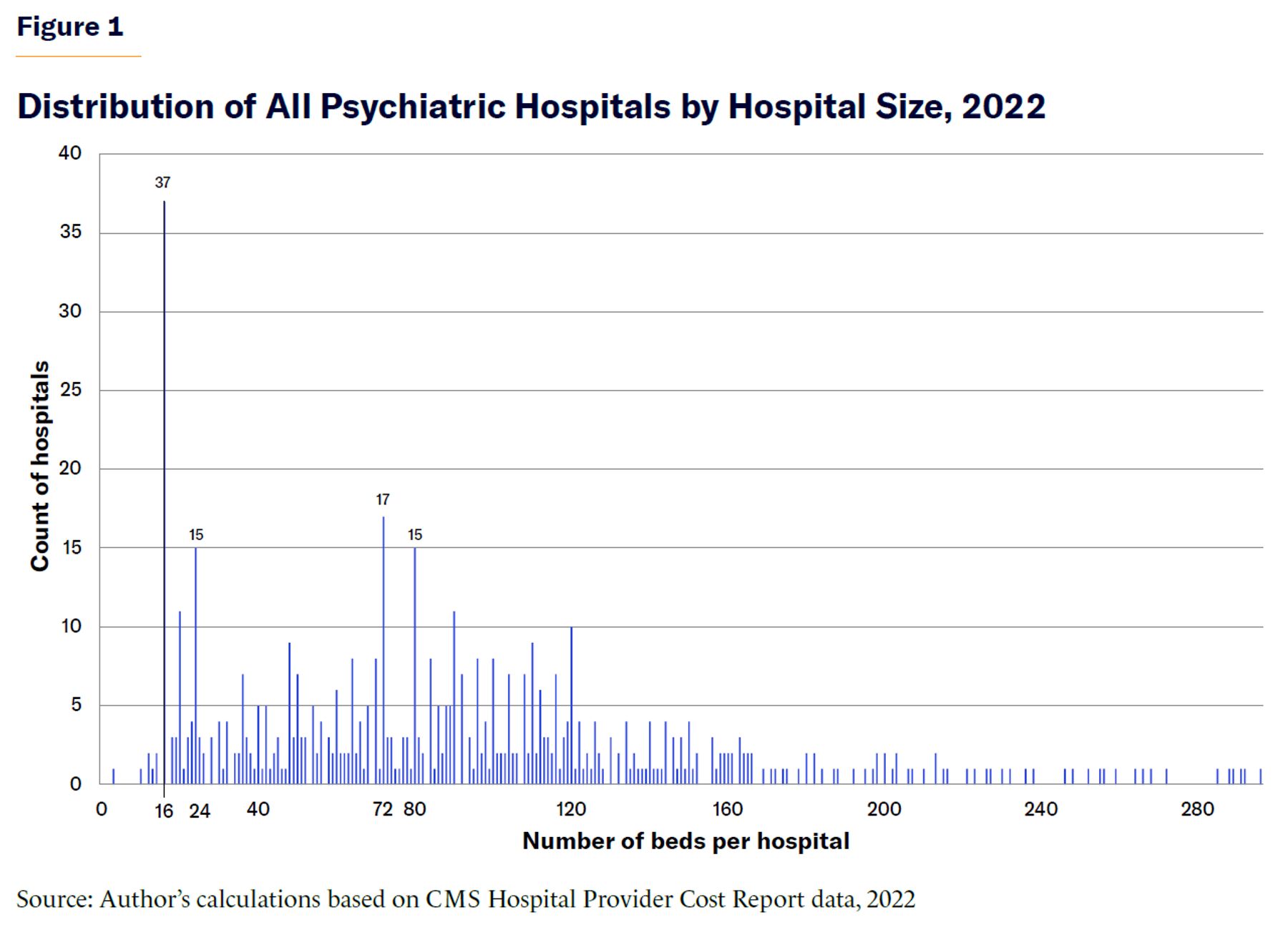
Figures 1 through 4 show distributions of hospitals by size and ownership. (For visual clarity, only hospitals with fewer than 305 beds are shown.) Public hospitals tend to be the largest, while for-profits are predominantly midsize hospitals and nonprofits are predominantly smaller hospitals. All distributions are right-skewed, meaning that more hospitals are smaller than the average hospital, rather than larger.
Figure 1 shows psychiatric hospitals of all ownership types by number of beds per hospital. A notable spike is seen at hospitals with exactly 16 beds, the size cap for FFP imposed by the IMD exclusion.
The 16-bed spike is most pronounced among public and nonprofit hospitals (shown in Figures 2 and 3, respectively), which suggests that these providers are most sensitive to the IMD exclusion.
Public hospitals have the longest right-tail distribution. As providers of last resort, these mostly state-run hospitals can be least flexible on size. Some minimum inpatient capacity must be provided by states to treat forensic patients, given legal obligations for competency restoration.
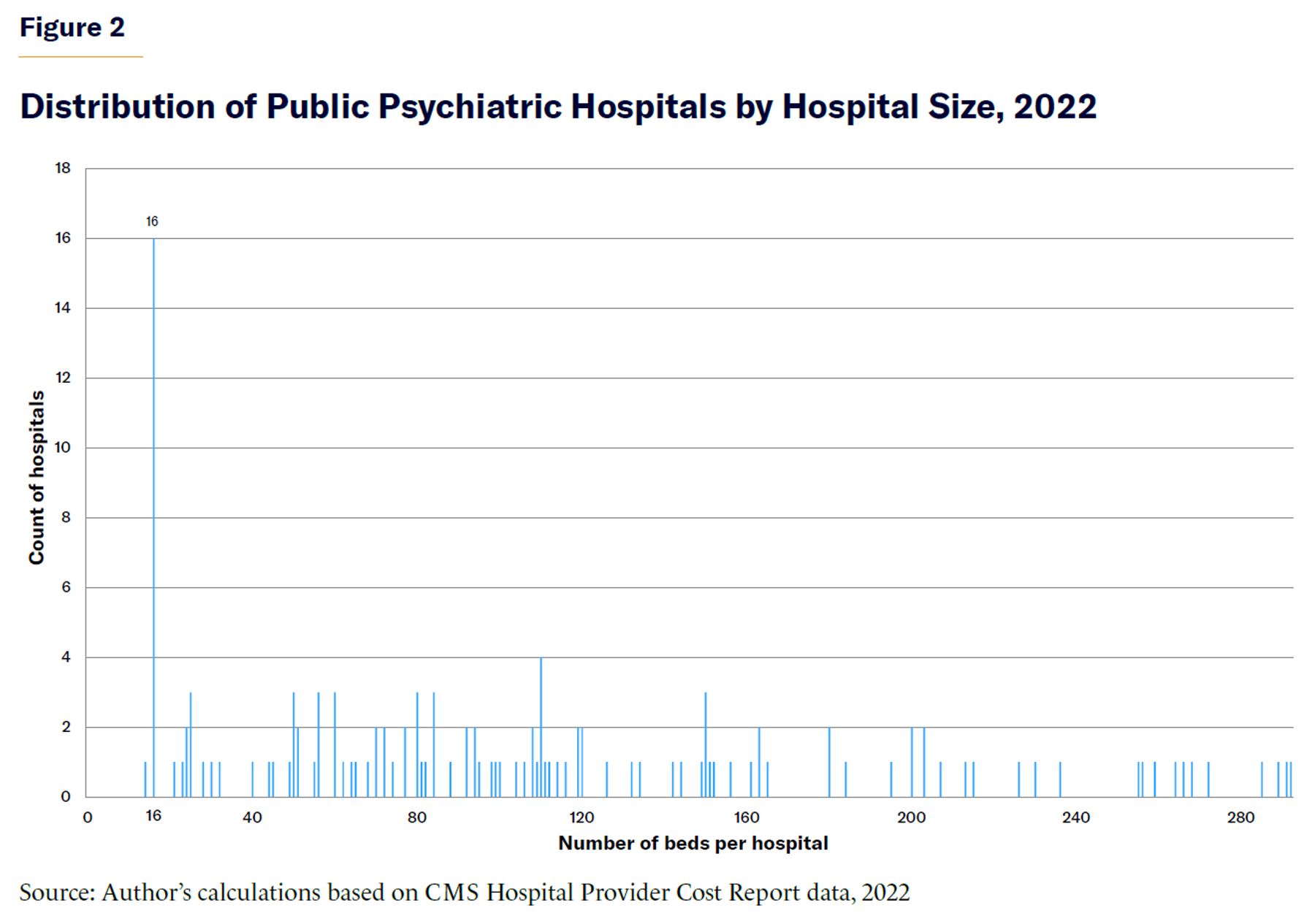
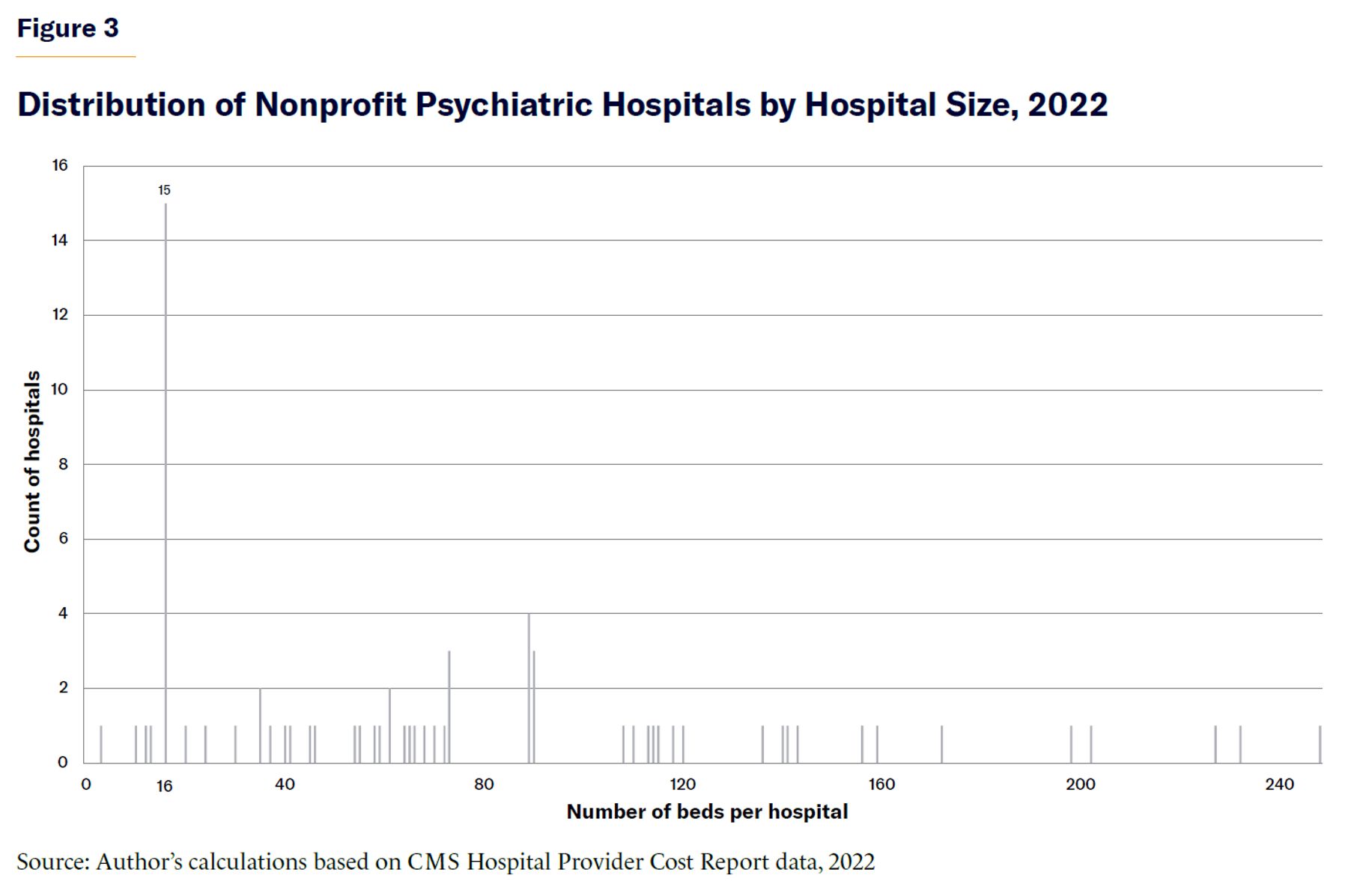
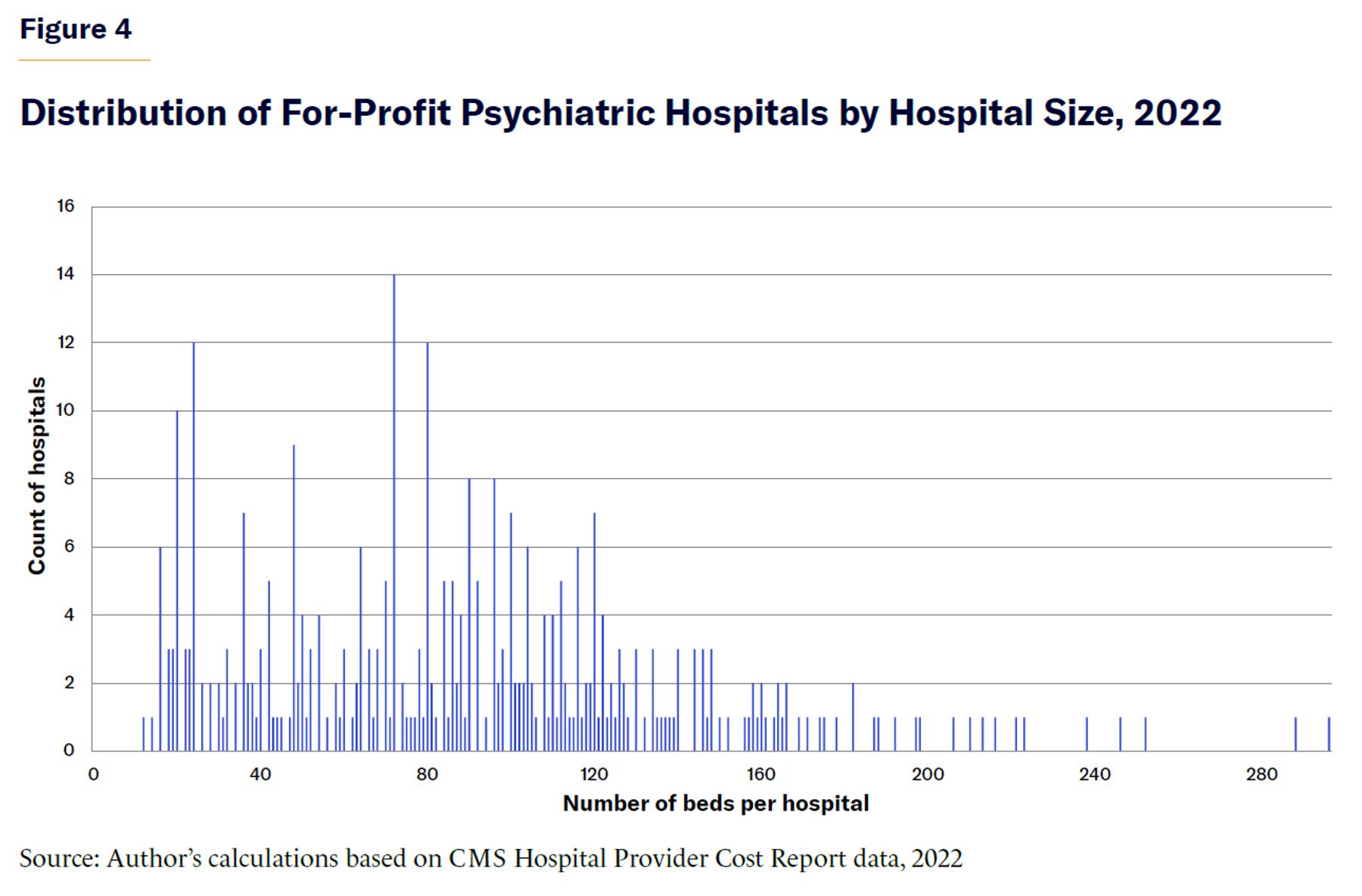
Figure 4 shows for-profit psychiatric hospitals, which greatly outnumber public and nonprofit hospitals. Their distribution peaks at 72 beds. For-profits are least subject to the IMD exclusion and least reliant on Medicaid patients, as they can attract privately insured patients whose care is often reimbursed at higher rates. Other spikes appear among for-profit providers, representing clusters of certain hospital sizes.
The size distributions for all ownership types are spiky rather than smooth due to the ways in which psychiatric hospitals are financed and regulated, affecting the optimal scale at which providers operate. The spikes in the figures at 16 beds clearly reflect a response to the IMD exclusion. Hospitals are likely to scale in fixed increments due to required staffing ratios and licensing constraints, among other factors. Some states have thresholds for licensing fees or certifications that might incentivize hospitals to organize around these requirements.[39]
Psychiatric hospitals also face fixed costs. For example, they have to invest to meet ligature risk requirements (that is, removing all physical points by which a cord, rope, or other object could be attached for the purpose of hanging or strangulation). There are also extensive conditions of participation for psychiatric hospitals to be Medicare- and/or Medicaid-certified providers, [40] which are more onerous than what is required of general hospitals.[41] Some of these conditions were issued in the 1960s and no longer reflect today’s health-care delivery.[42] For example, Medicare-certified psychiatric hospitals are required to complete and maintain extensive clinician-drafted individualized treatment plans for each patient, updated more frequently and in greater detail than what is required at general hospitals. This may have been warranted in decades past, when patients were sometimes hospitalized for months or years, [43] but this requirement is now impractical and provides limited benefit to patients, given today’s average length of stay of under nine days.[44]
Figure 5 provides an alternative view of this distribution by grouping hospitals in size bins. Most hospitals have more than 16 beds, which is noteworthy for two reasons. First, Medicaid beneficiaries will not be covered at most existing psychiatric hospitals based on the IMD exclusion’s size restriction. Were the exclusion repealed, tens of thousands of existing beds would become available and covered immediately for beneficiaries. Second, because most hospitals operate with 73 to 144 beds, providers may have a revealed preference for this size in the current financial and regulatory environment.
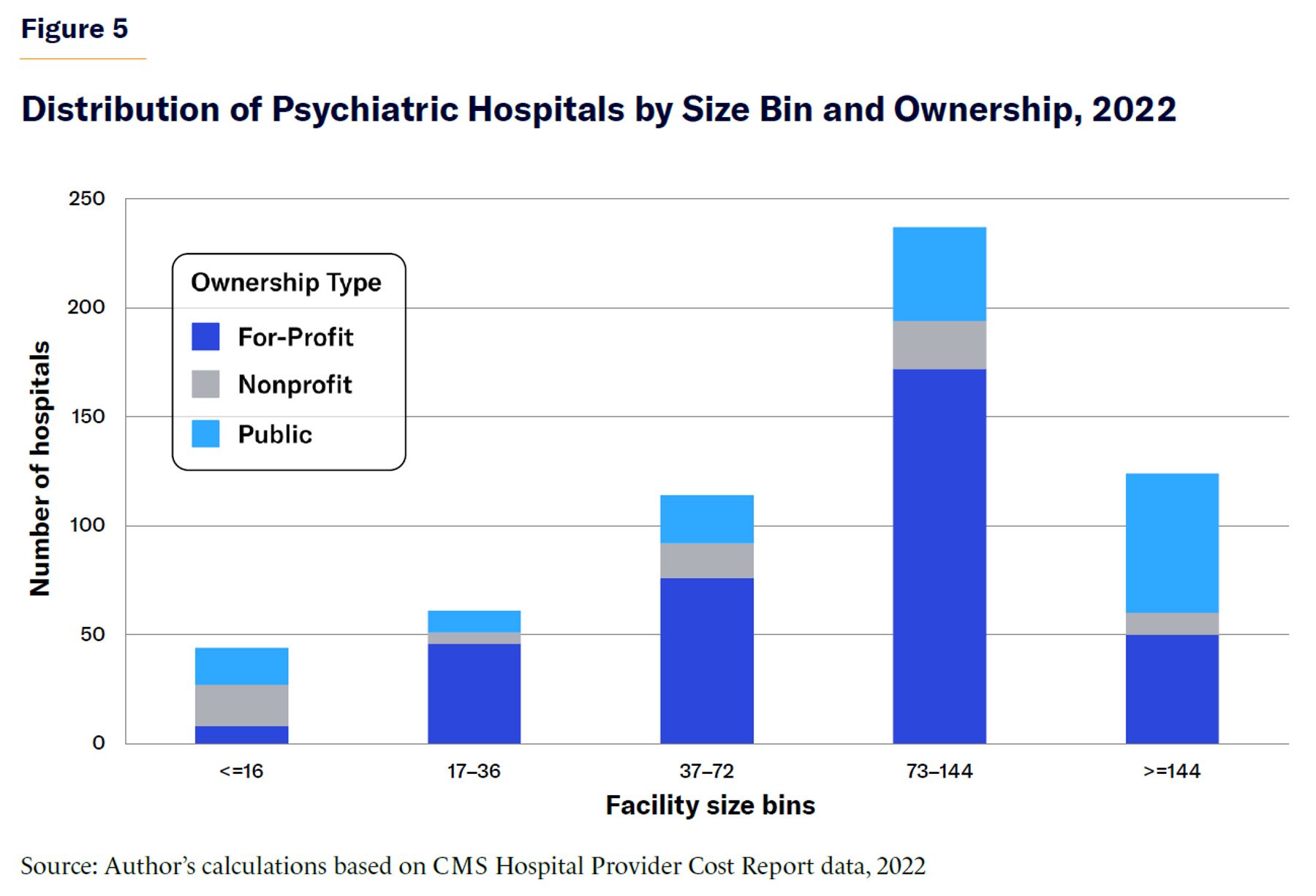
Most public hospitals have 144 beds or more, whereas that number of beds makes up the smallest share of nonprofit hospital capacity. To the extent that the IMD exclusion aims to avoid federal funding for the kind of custodial care more likely to occur in large state-run hospitals, the IMD-exclusion size threshold could still be significantly increased. A restriction on Medicaid funding for facilities with more than 144 beds would effectively continue to exclude those state hospitals without restricting other providers from being reimbursed for serving Medicaid patients.
Medicaid’s IMD exclusion means that hospital size dictates whether psychiatric hospital services can be covered. Repealing the IMD exclusion would allow Medicaid coverage for inpatient treatment at hospitals of any size—which is a necessary first step for increasing access. However, coverage alone does not guarantee that Medicaid beneficiaries will be served because hospitals can serve patients with Medicare or private health insurance, both of which typically reimburse hospitals at higher rates than Medicaid. To understand the extent to which IMD repeal may actually lead to more beneficiaries receiving treatment, it helps to examine how providers above and below the size threshold for FFP are currently serving Medicaid patients.
A high percentage of psychiatric hospitals in the N-SUMHHS data report accepting Medicaid.[45] Congruently, in the 2022 CMS Cost Report data, nearly 71% of all psychiatric hospitals (411 of 580) document at least one Medicaid-related discharge, meaning that a Medicaid beneficiary was discharged from an inpatient stay.[46] Table 2 shows the percentage and number of psychiatric hospitals reporting at least one Medicaid discharge for 2022.
Table 2
Hospitals Reporting at Least One Medicaid Discharge, by Size and Ownership
| Size | Ownership | % Reporting at least one Medicaid discharge | Number of hospitals |
| ≤ 16 beds | All | 75% | 33 |
| Public | 94% | 16 | |
| For-Profit | 38% | 3 | |
| Nonprofit | 74% | 14 | |
| 17+ beds | All | 71% | 536 |
| Public | 76% | 106 | |
| For-Profit | 72% | 38 | |
| Nonprofit | 68% | 106 |
Source: Author’s calculations based on CMS Hospital Provider Cost Report data, 2022
Although less than 8% of hospitals have 16 or fewer beds (and thus are eligible for Medicaid coverage), most hospitals report at least one Medicaid discharge. One explanation for this is the existence of various exceptions to the IMD exclusion, which will be described in the following section.
Another explanation for these discharges is the 1986 Emergency Medical Treatment and Active Labor Act (EMTALA), which requires Medicare-certified providers to furnish emergency services regardless of patients’ ability to pay. Most psychiatric hospitals participate in Medicare,[47] which under Part A covers treatment at psychiatric inpatient facilities with a 190-day lifetime limit, using a per-diem prospective payment system (IPF PPS) that adjusts for patient and facility characteristics.[48] Thus, the practical effect of EMTALA is that most psychiatric hospitals must admit or accept transfers of Medicaid patients with psychiatric emergency conditions (being homicidal, suicidal, or a danger to oneself or others). For hospitals with more than 16 beds, the result is uncompensated care.
While most psychiatric hospitals report at least one Medicaid discharge in 2022, Medicaid discharges are a small fraction of all discharges. Table 3 shows the percentage of Medicaid discharges among hospitals reporting at least one. (Medicare discharges are also shown for comparison.) Medicaid discharges make up 20% of all discharges among ≤16-bed psychiatric hospitals but only 4% of all discharges in larger hospitals.
Table 3
Median Percentage of Medicaid and Medicare Discharges Among Hospitals Reporting at Least One Medicaid Discharge, 2022
| Payer Type | Size | Ownership | |||
| All | Public | For-Profit | Nonprofit | ||
| Medicaid | ≤ 16 beds | 20% | 61% | 47% | 9% |
| 17+ beds | 4% | 11% | 2% | 10% | |
| Medicare | ≤ 16 beds | 10% | 13% | 8% | 8% |
| 17+ beds | 6% | 7% | 6% | 8% | |
Note: The high percentage of Medicaid discharges at small for-profit hospitals shown in Table 3 reflects a group of only three hospitals.
Source: Author’s calculations based on CMS Hospital Provider Cost Report data, 2022.
Past Experience of IMD Exclusion Modifications
Since its 1965 enactment, the IMD exclusion has been modified several times, including the regulatory definition (codified in 1988) allowing FFP at hospitals with 16 or fewer beds.[49] This size restriction represented a preference for short-term stays in community-based settings, rather than longer-term stays more typical of nursing homes and mental hospitals.[50]
The Social Security Amendments of 1972 exempted children under 21 from the IMD exclusion (and states have always had the option to exempt patients over 64).[51] Allowing IMD coverage for youth initially resulted in a significant expansion of psychiatric hospitals, given the new revenue potential.[52] However, patients with age-based exemptions account for very few psychiatric hospitalizations in IMDs or otherwise; 83.8% of psychiatric hospitalizations are for patients 18 to 64 years old,[53] and the rate of stays for the nonexempt age group is at least twice as high as for those who are exempt.[54]
There have been several recent (and bipartisan) changes to the IMD exclusion, including many since the first Trump administration. First, states with Medicaid managed-care plans can now make capitation payments to managed-care organizations (MCOs) for IMD care “in lieu of” services covered under a state plan if services are a clinically appropriate and cost-effective substitute, and if the IMD stay is under 15 days during the month of payment.[55]
Second, states can seek demonstration waivers under Section 1115 of the Social Security Act to cover short-term IMD stays for substance-use disorder (SUD)—made available by CMS in 2015, with guidance updated in 2017—and for serious mental illness (SMI) and serious emotional disturbances (SED) in youth, since late 2018.[56]
Third, since October 2019, the SUPPORT Act has allowed for a state option for Medicaid plans to cover SUD treatment in IMDs, for up to 30 days per year if several conditions are met.[57] Finally, while not technically an exemption, states can use a portion of Medicaid disproportionate share hospital (DSH) payments—which offset the cost of uncompensated care—to make lump-sum payments to psychiatric hospitals.[58]
Nearly every state makes use of at least one of these mechanisms (and some states make use of several) to draw down federal dollars for IMD services.[59] For example, among 41 states with Medicaid managed care, 31 used “in lieu of” authority in fiscal year 2020.[60] Fifteen states have Section 1115 waivers for SMI, and 37 have waivers for SUD.[61] Across 33 states, $2.9 billion in DSH payments were made to mental-health treatment facilities including IMDs in FY 2019.[62]
In 2023, a Congressional Budget Office (CBO) report examined Medicaid claims for SUD patients, finding that among states with Section 1115 SUD waivers, more IMD stays were reimbursed and more providers accepted Medicaid.[63] SMI waivers have been implemented more recently, and evaluations will be possible in the coming years.
Between 2012 and 2015, a federal demonstration project called the Medicaid Emergency Psychiatric Services Demonstration (MEPD) allowed FFP at participating private psychiatric facilities, which would otherwise be excluded under the IMD rule, across 11 states and the District of Columbia for services rendered to beneficiaries with emergency psychiatric conditions.[64]
The evaluation of MEPD faced data limitations: in most states, only six months of data were available, which was insufficient to determine whether the program had led to increased inpatient access for Medicaid beneficiaries. However, in the one state with 18 months of available data, beneficiaries’ admission rates rose toward the end of the period—suggesting a genuine increase in inpatient access, albeit after a delay, possibly as providers became aware of, or adjusted to, the change.
Interviews with IMD staff during MEPD provided additional insight. In most states, staff said that they could not infer whether the demonstration affected discharge patterns, but only because “the facilities typically did not admit adult Medicaid beneficiaries before MEPD”[65] —a response that suggests that the demonstration did lead to greater access.
The MEPD evaluation also shed light on the limited effectiveness of waivers versus that of a full repeal. Many states stopped demonstration enrollment months in advance of the scheduled end out of fear that expected reimbursement might be withheld or that funding had run out. The changing (and political) nature of CMS decisions may prevent hospitals from opting to serve Medicaid patients—or add bed capacity—if there is lingering uncertainty about reimbursement.
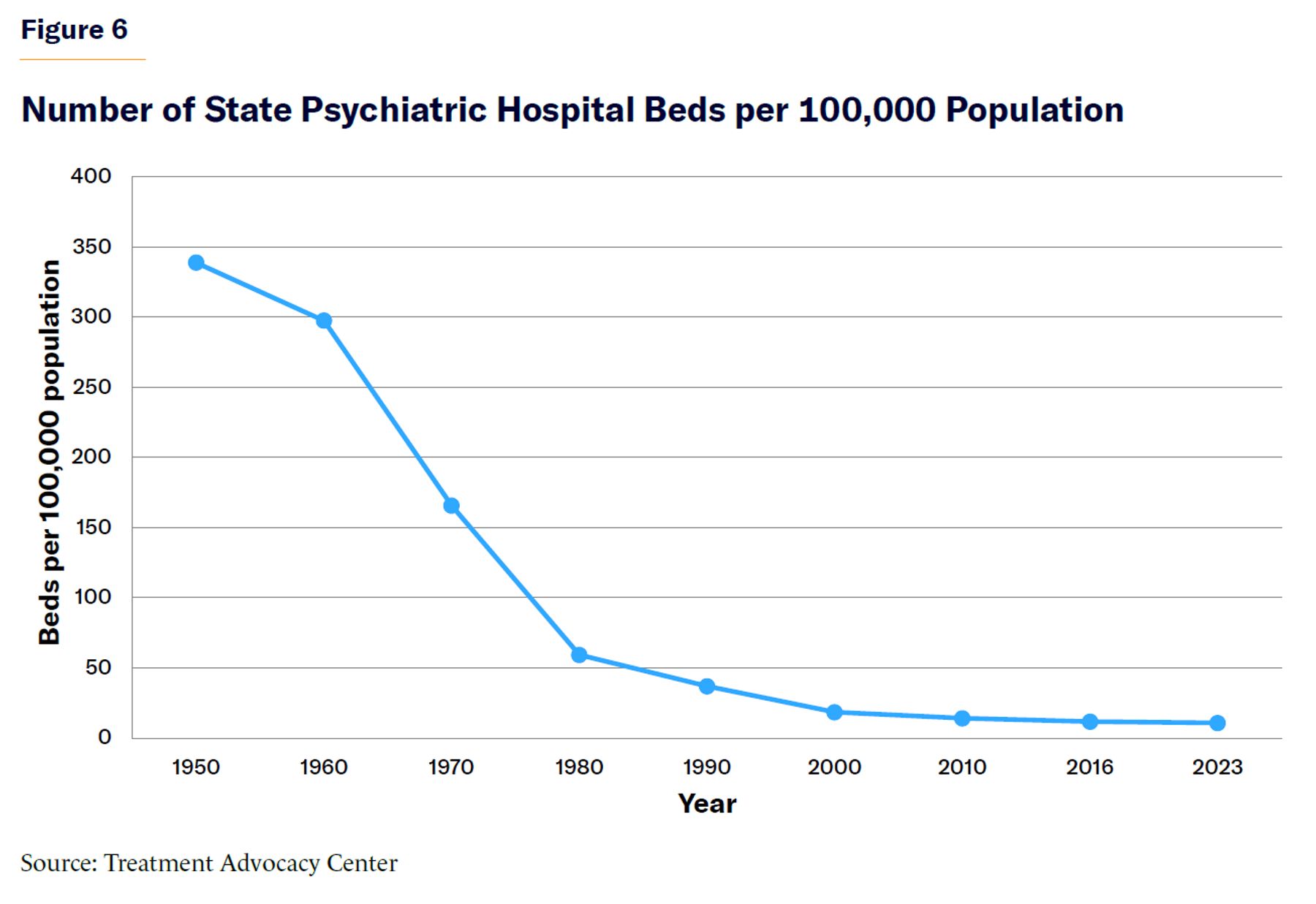
In summary, over the decades, there have been several modifications to the IMD exclusion that—despite being motivated by a desire for more inpatient capacity—have failed to reverse the downward trend of psychiatric hospital bed capacity. [66] This is especially clear among public providers, which serve the greatest share of Medicaid patients.[67] Figure 6 shows the decline in state psychiatric hospital beds per 100,000 from a peak in the 1950s.[68]
Ownership Dynamics of Psychiatric Hospitals
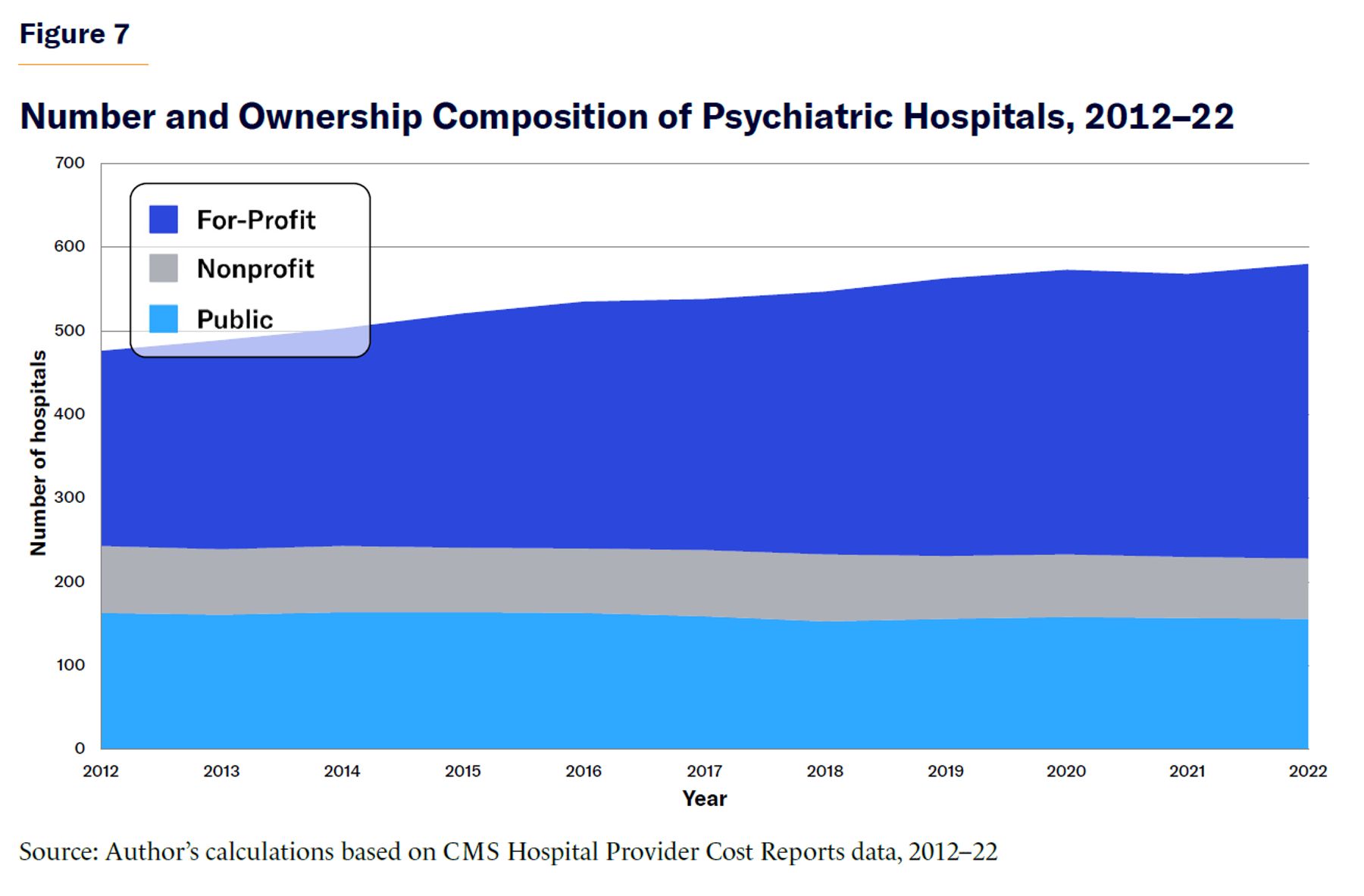
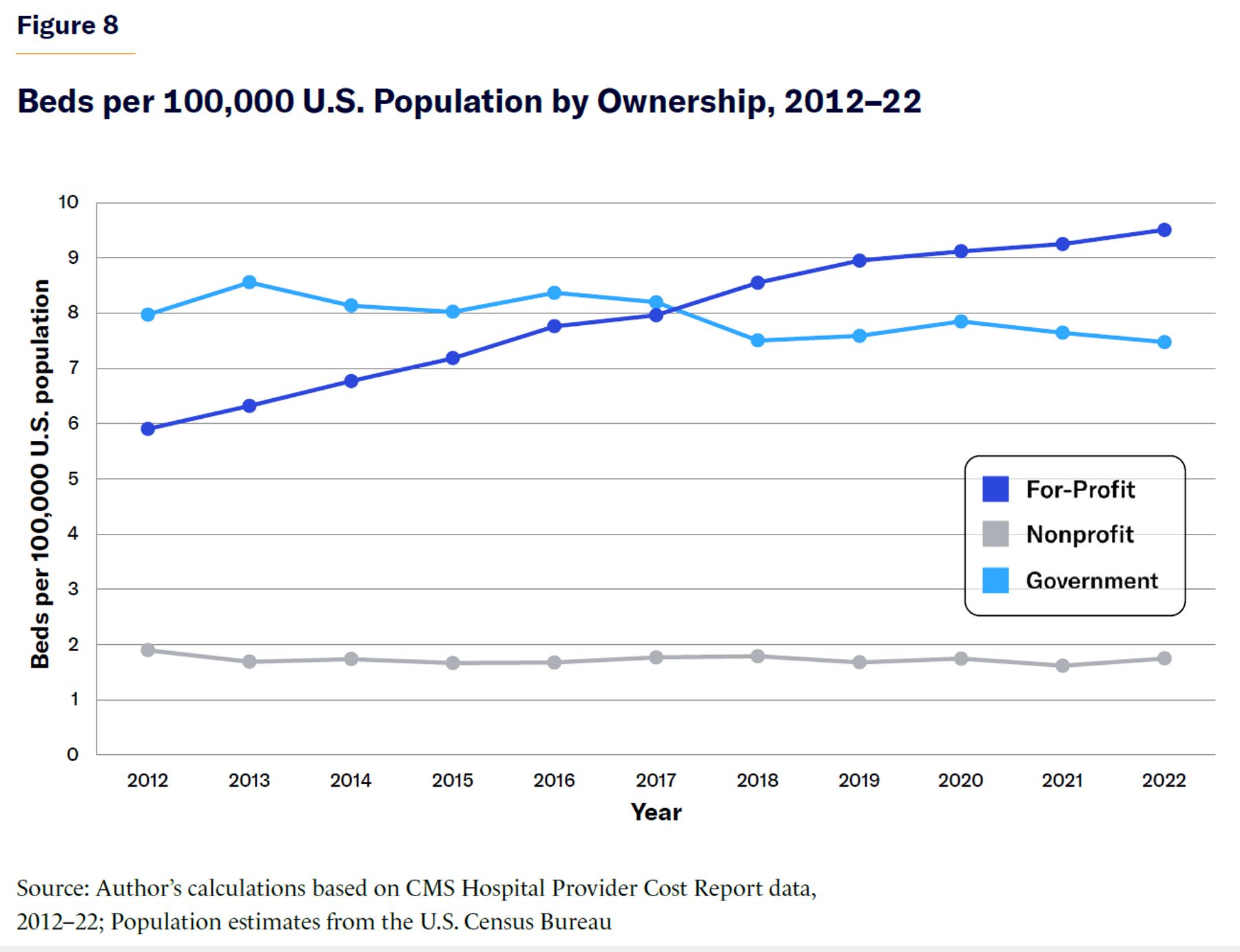
There is one exception to the general trend of declining inpatient psychiatric beds: the for-profit sector.[69] The number of for-profit psychiatric hospitals increased between 2012 and 2022 (shown in Figure 7), as did the number of for-profit beds (shown in Figure 8). Indeed, the growth of for-profit psychiatric hospitals—the most numerous ownership type—has led to an overall increase in the number of psychiatric hospital beds. However, other research has found that this growth in for-profit psychiatric hospitals has occurred alongside the decline in general hospital psychiatric bed capacity since 2004, suggesting that the total number of psychiatric beds across both psychiatric hospitals and general hospital psychiatric units has not increased.[70]
Usually, it is good to have more providers of inpatient psychiatric care, but a greater number of for-profit hospitals does not guarantee increased access to hospital care for seriously mentally ill Medicaid beneficiaries, the homeless, or the incarcerated. Over the last decade, as for-profit psychiatric hospitals have expanded, their share of Medicaid discharges has declined (Table 4). The overall share of psychiatric hospitals with more than 16 beds (hospitals directly affected by past-decade exemptions) that report at least one Medicaid discharge declined between 2012 and 2022, from 74% to 71%; among for-profit hospitals, that figure dropped from 72% to 68% (see Appendix Table A). Among the now-smaller share of over-16-bed hospitals reporting at least one Medicaid discharge, Medicaid discharges as a fraction of total discharges have also declined (Table 4).
Table 4
Median Percentage of Medicaid Discharges Among Hospitals Reporting at Least One Medicaid Discharge
| Psychiatric hospitals with 17+ beds | ||||
| Ownership | All | Public | For-Profit | Nonprofit |
| 2022 | 4% | 11% | 2% | 10% |
| 2021 | 6% | 10% | 3% | 10% |
| 2020 | 6% | 10% | 3% | 9% |
| 2019 | 7% | 10% | 5% | 9% |
| 2018 | 7% | 10% | 5% | 12% |
| 2017 | 8% | 8% | 5% | 9% |
| 2016 | 7% | 7% | 6% | 8% |
| 2015 | 7% | 7% | 7% | 13% |
| 2014 | 8% | 8% | 7% | 13% |
| 2013 | 8% | 7% | 7% | 12% |
| 2012 | 8% | 5% | 9% | 12% |
Source: Author’s calculations based on CMS Hospital Provider Cost Report data, 2012–22
As Table 4 shows, as for-profits served proportionately fewer Medicaid beneficiaries, public hospitals served proportionately more. However, it is important to emphasize that fewer than half of all beds are in public hospitals.
Inpatient psychiatric care is not a lucrative business. At least 37% of all psychiatric hospitals operate with negative net-profit margins—and patients on Medicaid are less lucrative than patients with other means to pay.[71] For-profit providers are essential to the mental-health system, but if policymakers want to expand inpatient access to seriously mentally ill Americans who are currently homeless or incarcerated, for example, for-profit provision will be of limited benefit.
To be sure, repealing the IMD exclusion does not change low Medicaid reimbursement rates, other than effectively “raising” them from the current rate of $0 (minus the cost to psychiatric hospitals of serving beneficiaries without compensation). Both repeal and increased Medicaid reimbursement rates may ultimately be necessary to encourage psychiatric hospital providers to add beds, let alone maintain current capacity.
Evaluating Current Proposals for Reform
Many policymakers now agree on the need for more psychiatric beds and that changing Medicaid’s IMD exclusion is necessary to make that happen.
One such change to the IMD exclusion—featured in a bill that was previously introduced in the House of Representatives—would increase the size threshold for an IMD from more than 16 beds to more than 36 beds. But as Figure 9 shows, such a change would likely have little impact on Medicaid beneficiaries’ access to inpatient services because there are few hospitals with 36 beds or fewer that could benefit from such a proposal.
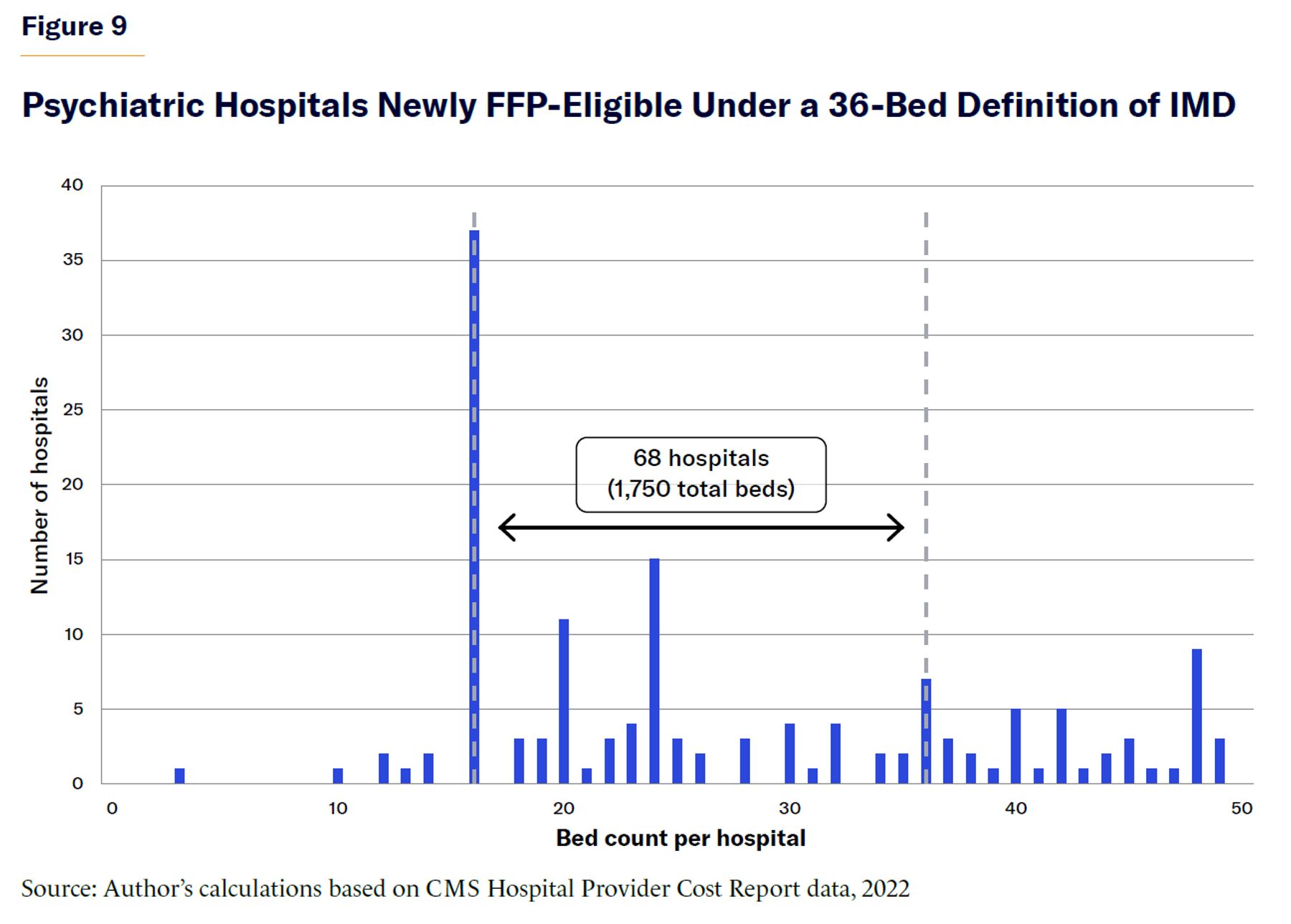
Assuming that psychiatric hospitals are still operating at the same size as in 2022, raising the threshold to 36 beds would result in only 68 additional psychiatric hospitals (with 1,750 beds) gaining access to Medicaid funds, at most.[72] Fifteen of those hospitals (401 beds) are public (10 hospitals) or nonprofit (5 hospitals). While it’s uncertain how many providers would enter the market anew under such a threshold, expectations should be tempered, given that few hospitals operate within this size range.
If all hospitals with between 16 beds (exactly on the cusp of the current restriction) and 35 beds increased in size to meet the new threshold—an overly generous assumption—the result would be only 594 additional beds (on top of the newly covered 1,750). Furthermore, these already-minimal benefits may be further reduced if hospitals with just over 36 beds took beds offline to meet the new threshold. Fourteen hospitals have between 36 and 41 beds, with a total of 40 beds that could be reduced across facilities to meet the 36-bed threshold.
Given that there are more than 100,000 seriously mentally ill homeless Americans[73] and hundreds of thousands of incarcerated seriously mentally ill Americans, it is doubtful that several hundred more beds serving Medicaid beneficiaries would make a noticeable impact on America’s mental-health crisis.
Because the vast majority of psychiatric hospitals have between 73 and 144 beds, a hypothetical definition change allowing FFP at IMDs within this higher range is worth examining. Figure 10 shows the number of hospitals that would become covered under a hypothetical 108-bed threshold—the midpoint of 73 and 144 and the average size of all psychiatric hospitals.
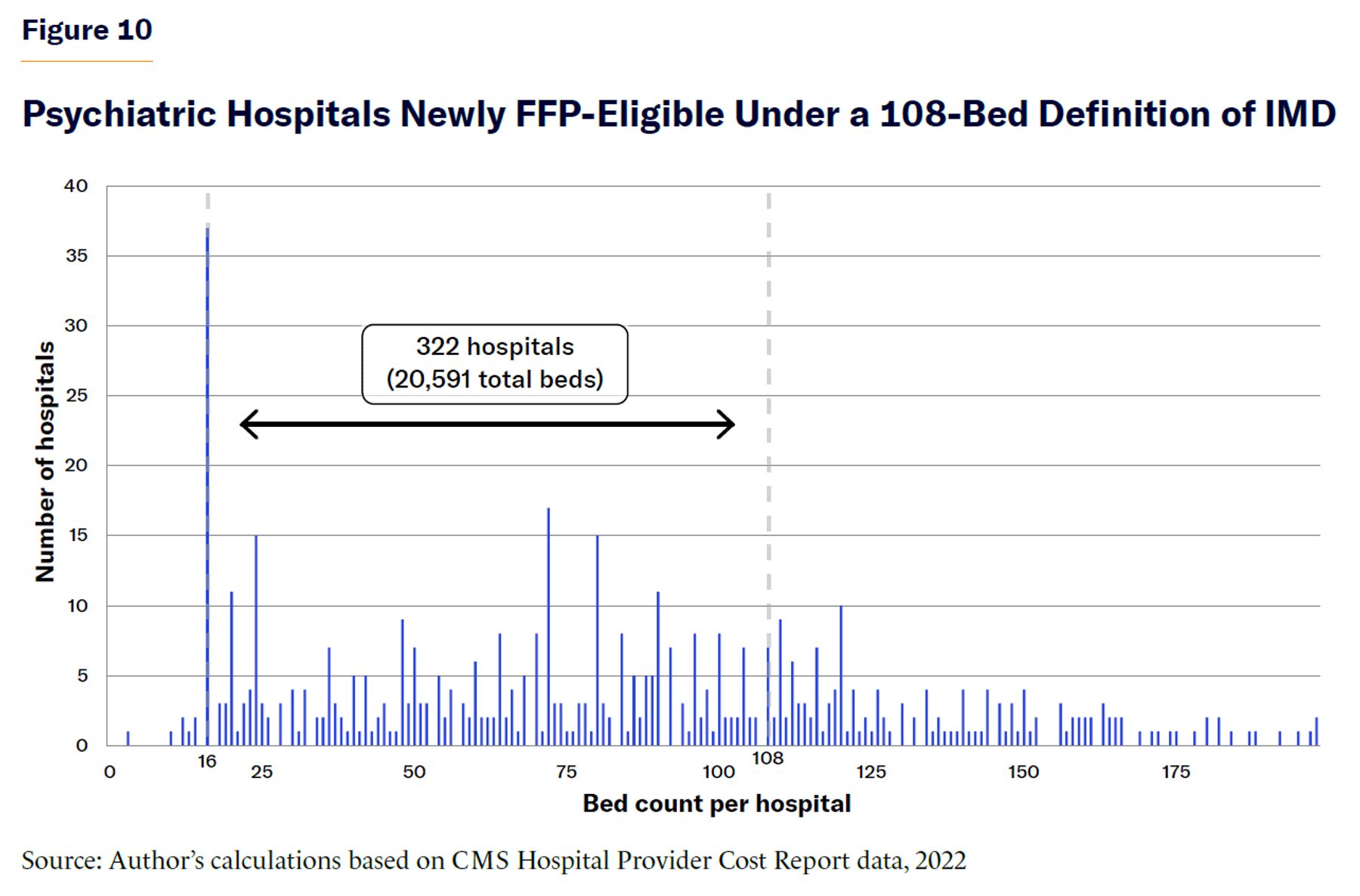
An increase in the size threshold to 108 beds would allow a far greater number of hospitals to become covered settings—322 hospitals total, including 58 public hospitals and 33 nonprofit hospitals, for a total of 20,591 beds newly covered under Medicaid. If all hospitals operating in 2022 with between 16 (inclusive) and 107 beds were to increase their size to meet the new 108-bed threshold—again, an overly generous assumption—the result would be an additional 15,439 beds (on top of the 20,591).[74] This reform is far more likely to meaningfully increase Medicaid beneficiaries’ access to necessary inpatient care, though still inferior to full repeal.
Figures 9 and 10 represent rough estimates of the number of psychiatric hospitals and beds that would no longer be excluded from Medicaid based on size. Hospital ownership and other factors affect the extent to which beds that become newly available to Medicaid patients would ultimately serve them—as well as the extent to which current providers would expand or new providers would enter the market. These ranges, therefore, are not definitive, but they do represent the potential impact of broader IMD exclusion reforms, if full repeal is not possible.
Considering the Cost of Repeal
The best argument for modifying, rather than simply repealing, the IMD exclusion is the fiscal impact of the latter.[75] Rising Medicaid costs are a challenge about which policymakers are right to be concerned, and policymakers may want to consider ways that less effective mental-health spending can be reduced to offset costs to IMD exclusion repeal. While a full cost analysis of repeal is beyond the scope of this report, some considerations are worth discussing.
In fiscal year 2019, the U.S. spent $43.2 billion on all IMD- and non-IMD-based inpatient treatment for mental health and substance abuse. Medicaid accounted for $19.3 billion of that spending.[76] For 135,502 individuals treated in state psychiatric hospitals in fiscal year 2019, Medicaid contributed $2.1 billion (of combined state and federal Medicaid funds) out of a total of $11.5 billion spent. State revenue from general funds and special funds account for essentially all the rest ($9.3 billion).[77] (The total per-patient cost in state hospitals that year was $84,748, on average.) In the 2012–15 MEPD, the average amount claimed per admission to a private psychiatric hospital was $6,766.[78]
Absent explicit cost-neutrality requirements, repealing the IMD exclusion would mean new costs for the federal government because services not previously eligible for FFP would become eligible. But the important question is whether these costs are outweighed by the benefits. There is an obvious cost to society of leaving serious mental illnesses inadequately treated: greater homelessness, incarceration, public disorder, and violence. Policymakers wary of IMD-exclusion repeal due to the cost may find that inaction presents less cost savings than expected.
In 2023, CBO estimated the cost to the federal government of IMD-exclusion repeal for mental-health stays to be about $3.3 billion per year over 10 years.[79] However, even absent repeal, CBO noted that the federal government would still incur much of this cost, as states increasingly make use of waivers to cover patients. At the time of CBO’s estimate, one state had a Section 1115 waiver for mental health, and 25 states had an 1115 waiver for SUD, with 73% of Medicaid enrollees aged 21 to 64 living in states with waivers. Today, 15 states have mental-health waivers, and 37 states have SUD waivers, both of which allow for coverage of short-term IMD stays.
Another reason that IMD repeal would be less expensive than many assume is that the vast majority of IMD stays are short-term. The median length of stay for Medicaid beneficiaries in the MEPD demonstration was seven days (with an average of 8.6 days). Nearly 90% of all stays were under 32 days. These metrics are consistent with CBO’s admission that many IMD stays will become covered and paid for with federal dollars absent any legislative action. Only 1,300 Medicare beneficiaries reached the 190-day lifetime limit in 2023,[80] so for the vast majority of Medicaid patients, stays will be short-term.[81] Shorter lengths of stay are, in part, a function of Medicaid plans increasingly operating under managed-care models,[82] which act as a check against unnecessarily long inpatient stays.[83]
Furthermore, although inpatient treatment for serious mental illness is inherently expensive, IMDs can provide more cost-effective services. For patients with psychiatric emergency conditions, for example, the average price of all emergency-room services in 2021 was over $5,550 per admission.[84] Multiple or repeated stays in the ER may cost more than a single admission to a psychiatric hospital, which is a more effective and clinically appropriate setting. For this reason, CBO estimated that reductions in ER use would partially offset some of the cost of IMD repeal.
As the number of dedicated psychiatric beds in general hospitals decreases, patients are increasingly treated in “scatter beds,” which are not dedicated to or equipped for psychiatric treatment. More treatment in scatter beds will only further increase the cost of treatment in general hospitals as compared with specialty hospitals.
Finally, it’s worth noting that the IMD exclusion was intended to prevent cost-shifting of mental-health care from states to the federal government, but it has failed to do so: the federal share of spending on mental health has vastly increased compared to state spending since the enactment of the IMD exclusion.[85] States have simply shifted spending away from psychiatric hospitals and toward Medicaid-covered services that capture federal dollars and meet states’ federally required matching payments.[86] Because patients with serious mental illness are most likely to need hospitalization not covered by Medicaid, mental-health dollars have instead been spent on those with less serious functional impairment. In short, the result has been to encourage greater utilization of mental-health services by a population less in need.[87]
In terms of cost-shifting, repealing the IMD exclusion need not happen in a vacuum. Proposals have been made to eliminate the open-ended federal matching that currently exists.[88] Capping the federal matching allocation to states for Medicaid-covered services—but removing the discrimination against the IMD setting—would do more to contain Medicaid costs overall than keeping the IMD exclusion in place.
A combination of repealing the IMD exclusion and placing an upper-limit cap on Medicaid matching would be a reasonable scenario: repealing the IMD exclusion would remove any distortion it creates in dictating service setting—distortions that clearly exist, given the many work-arounds that states take advantage of currently to draw down federal dollars for IMD care—but growth of the overall Medicaid program would be necessarily reined in. To the extent that IMD care is less expensive than other settings, such as general hospital psychiatric units, this would also provide a more economical option for care. Finally, a cap with no IMD exclusion would allow states better discretion to prioritize services most needed in each individual state; this may help allocate resources toward seriously mentally ill individuals most in need.
Conclusion
The IMD exclusion restricts Medicaid beneficiaries from receiving inpatient psychiatric treatment in IMDs such as psychiatric hospitals—a limitation that does not exist for any other type of treatment setting. As of 2018, half of all beneficiaries with serious mental illness reported unmet needs.[89] Not meeting those needs has consequences not only for patients themselves but also for the public in the form of higher rates of homelessness, incarceration, public disorder, and violence.
The amount of public disorder and violence that comes from untreated mental illness is a policy choice. There are psychiatric hospitals currently operating that could serve individuals with serious mental illnesses if doing so were financially feasible. But prohibiting reimbursement for treatment in psychiatric hospitals—without any clinical justification—exposes hospitals to financial losses from uncompensated care, a risk that becomes unavoidable as hospitals grow beyond 16 beds.
Over the past decade, various mental-health reforms have garnered bipartisan support, suggesting that congressional action on the IMD exclusion is politically feasible. While appetite for full repeal has been limited in the past, momentum appears to be growing: lawmakers, researchers, practitioners, and advocacy organizations—across partisan lines—have called for repeal.[90] The Trump administration has also publicly indicated support for addressing the IMD exclusion and expanding the use of psychiatric hospital settings.[91]
Coverage for serious mental illness at scale is necessary to address the lack of access to inpatient psychiatric care. The slow but steady rate of decline among public and nonprofit hospitals over the last 15 years suggests that IMD-exclusion repeal may be necessary simply to keep hospitals in operation at their current capacity.
Acknowledgments
The author would like to thank Ken Locey, especially, for guidance and assistance related to CMS Hospital Provider Cost Report data. The author would also like to thank Stephen Eide, Scott Dziengelski, Sherry Glied, Judge Glock, Chris Pope, Elizabeth Sinclair Hancq, Cheryl Roberts, and Ryan Aminloo for their valuable insights.
Appendix
Data Description
This report examines freestanding psychiatric hospitals, as CMS Hospital Provider Cost Report data do not cover all IMD-designated facilities, such as residential-treatment facilities. Some residential treatment facilities are present in the data if they operate inpatient units accredited or licensed as psychiatric hospitals. However, distinguishing residential-treatment facilities from psychiatric hospitals, which require manual corroboration against public information, is not done here.[92] Non-IMD general hospital psychiatric beds (FFP-eligible) are also excluded, as they are indistinguishable within bed counts of each general hospital record.
Cost-report data are generated via annual forms that all Medicare-certified institutional providers submit to CMS.[93] CMS requires all Medicare-certified institutional providers to complete cost reports or risk losing federal funds. The data describe characteristic information for hospitals, including type (corresponding to the primary health-care services provided—children’s hospitals, psychiatric hospitals, etc.), ownership (e.g., public versus private), and size (e.g., number of beds). The vast majority of psychiatric hospitals are Medicare-certified, making the cost report data relevant and useful. [94]
This report primarily uses publicly available 2022 CMS Hospital Provider Cost Report data, with some analyses drawing on data back to 2012.[95] A total of 630 psychiatric hospital records are included in the 2022 data, 580 of which are unique hospitals with non-null bed counts reporting at least one inpatient discharge (used to confirm that inpatient services are provided). Those 580 psychiatric hospitals account for 62,439 beds in operation. Compared with other benchmarks, total hospital and bed counts are in line with American Hospital Association reports[96] and higher than the 2022 N-SUMHHS (481 hospitals, 48,038 beds), possibly due to inclusion of some residential-treatment facilities, which are counted separately in the N-SUMHHS.[97]
A record was deleted from data analyzed if it: (1) was not identified as a psychiatric hospital, (2) did not have a total bed count listed per hospital or facility, (3) did not have at least one inpatient program day, or (4) was a duplicate hospital within any given reporting year. In time series analyses, not all hospitals were present each year. Hospital ownership was determined as “for-profit,” “nonprofit,” or “government” based on a created grouped indicator of ownership types. An indicator was created for records where at least one Medicaid-related discharge was reported (Title XIX). All records had at least one Medicare-related discharge (Title XVIII), so no indicator was needed. The percentage of Medicaid discharges per record was calculated as the number of Medicaid-related discharges (Title XIX discharges) reported in a given record over the number of total discharges reported in a given hospital record. Analyses were conducted using Python.
Appendix Table A
Percentage and Number of Hospitals Reporting at Least One Medicaid Discharge, by Size and Ownership
| <= 16 beds | 17+ beds | |||||||
| All | Public | Nonprofit | For-Profit | All | Public | Nonprofit | For-Profit | |
| 2022 | 75% (33) | 94% (16) | 74% (14) | 38% (3) | 71% (536) | 76% (106) | 72% (38) | 68% (106) |
| 2020 | 72% (33) | 88% (15) | 71% (15) | 38% (3) | 70% (367) | 72% (101) | 70% (38) | 69% (228) |
| 2018 | 78% (39) | 94% (16) | 75% (18) | 56% (5) | 70% (348) | 74% (100) | 64% (36) | 70% (212) |
| 2016 | 79% (42) | 94% (16) | 83% (19) | 54% (7) | 66% (316) | 75% (109) | 61% (33) | 62% (174) |
| 2014 | 76% (39) | 94% (17) | 67% (14) | 67% (8) | 70% (317) | 77% (112) | 69% (40) | 67% (165) |
| 2012 | 80% (37) | 93% (14) | 76% (16) | 70% (7) | 74% (319) | 79% (117) | 71% (42) | 72% (160) |
Source: Author’s calculations based on CMS Hospital Provider Cost Report data, 2012–22
Endnotes
Photo: Luis Alvarez / DigitalVision via Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).