Untangling the Hospital Safety Net

Photo: JazzIRT/iStock
Introduction
In order to fund emergency health care for indigent patients, the U.S. provides billions of dollars in subsidies to hospitals. But these subsidies allocate aid to facilities that need it least, fail to protect indigent patients from high charges, and cost substantially more than the total value of free and discounted care provided to the uninsured.
Hospitals in 2019 provided $42 billion in medical care for which they were not paid in full, but every year they receive about $49 billion in public funds for the purpose, mostly as add-on payments to Medicare and Medicaid. Thus, hospitals alone received an average of $1,788 per uninsured U.S. resident—$761 more than the average level of uncompensated care that the uninsured received from all medical providers.
Federal subsidies nonetheless prove inadequate for many facilities because funds are distributed senselessly: in 2023, for the largest type of hospital subsidy, New Hampshire received $2,123 per poor resident; Wyoming, only $4. Within states, the distribution is just as arbitrary, and funds are often provided without any requirement that additional services will be delivered in return.
To untangle the hospital safety net, federal aid for hospitals should be consolidated into grants that are distributed in proportion to the value of free and discounted care that each facility provides to low-income uninsured patients, up to a cap. In return for accepting these funds, hospitals should accept limits on charges and collections from uninsured patients.
Treating the Uninsured
Over the past century, rising affluence and medical innovation have rapidly increased demand for health insurance to improve access to cutting-edge care.
As medical technology advanced, the range and cost of hospital services rose rapidly. Following World War II, the American Hospital Association lobbied for federal funds to compensate it for treating patients unable to pay for themselves.[1] From 1950, Congress provided matching funds for states to aid providers furnishing medical services to welfare recipients; and in 1965, Congress established Medicare and Medicaid to directly provide coverage to elderly and low-income Americans.[2]
Medicare and Medicaid substantially reduced the number of uninsured low-income patients, the out-of-pocket cost exposure of beneficiaries, and the uncompensated care burden on hospitals.[3] But because the federal government paid hospitals according to the costs of delivering care to Medicare and Medicaid patients, expenses surged.[4]
The share of hospital revenues from out-of-pocket payments fell from 50% in 1950 to 3% in 2021.[5] The expansion of private insurance and public entitlements drove up the intensity and cost of hospital care, causing the average cost per patient day to soar from $5.42 in 1935 to $2,883 in 2021 (an amount 28 times higher, after accounting for general inflation).[6]
In 2021, 56% of the U.S. population were covered by private insurance, while 35% were enrolled in Medicare, Medicaid, or other public programs.[7] That left 8% of all U.S. residents uninsured, generally because they were unable to afford insurance and were ineligible for entitlements. A total of 17% of those with incomes below the poverty line, 16% of those living in states that didn’t expand Medicaid under the Affordable Care Act, and 30% of noncitizen residents lacked health insurance.[8]
As insurance and entitlement programs have become dominant, arrangements for the uninsured have fallen into neglect. In the past, hospitals charged wealthy patients more, in order to cross-subsidize the poor; now, they charge patients paying out-of-pocket prices slightly more than they do insurers for the same medical procedures.[9]
The uninsured enjoy less access to care and are exposed to higher out-of-pocket costs when they receive it. According to the Medical Expenditure Panel Survey, in 2021 individuals with insurance consumed, on average, $7,278 in health-care services (and paid $934 out of pocket), while the uninsured averaged $1,639 in expenditures (and paid $612). Whereas 6.0% of Americans were admitted to a hospital, only 1.6% of the uninsured received inpatient treatment. Among those who had inpatient expenses, the insured received an average of $21,710 in inpatient services (and paid $547 out of pocket), while the uninsured received $13,480 (and paid $2,265 out of pocket).[10]
To compare patterns of care and payment in unanticipated hospitalizations, a 2005 study analyzed patients suffering major car accidents, finding that the uninsured received 20% less care, and were 39% more likely to die, than those with private insurance coverage.[11]
Because costly emergency hospitalizations are not planned and the uninsured generally lack the savings to pay all at once, they are a major contributor to the debt burden on low-income Americans, who wouldn’t typically gain access to large unsecured commercial loans.
Medical debt is highly concentrated among a small minority of the population: 0.3% of adults account for more than half of it.[12] Whereas only 1.7% of Americans owed over $5,000 in medical debt in 2022, 4.2% of the uninsured did—with a mean of $29,029 owed by uninsured debtors.[13] Given that the uninsured typically have virtually no liquid savings, this can lead to disaster.[14] For those with health insurance, the four-year bankruptcy rate increases from 3.4% to 3.8% after hospitalization; for the uninsured, it leaps from 3.7% to 5.1%.[15] Part of this effect is likely due to lost wages during the post-hospitalization period of ill health.
Hospitals send 51% of medical bills run up by the uninsured to collections, but they recover only 9% of the face value of debts within two years. Repayment rates are low for medical debts exceeding $1,000.[16]
A study of the 100 largest hospitals in the U.S. from 2018 to 2020 found that 26 pursued court actions for unpaid medical bills, seeking an average repayment of $1,842.[17] A study of Texas hospitals from 2018 to 2020 found that 7% of them sued for unpaid bills, yielding an average 0.15% of hospital revenues—with the uninsured accounting for about half the lawsuits. One patient with a five-day hospital stay following emergency surgery was successfully sued for $200,000 in unpaid bills, legal fees, and 5% interest—amounting to seven times his annual income.[18]
The provision of free and discounted hospital care to the uninsured serves as a partial substitute for the purchase of insurance. For the first $2,000 of medical services that they consume in a year, the uninsured pay out-of-pocket amounts similar to those with insurance, but when they receive more than $2,000 in medical care, they typically bear little additional expense.[19] Overall, the uninsured pay for only 20%–35% of the cost of care that they receive.[20] Nationwide, hospital debts in collection are increasingly excluded from credit reports.[21]
One study estimated that low-income uninsured Americans are willing to pay less than a third of expected health-care costs to purchase health insurance. Above the income cutoff for eligibility for free and discounted care, the willingness to pay for insurance was significantly greater.[22] Uninsured households in states that exempt more assets from seizure in bankruptcy are significantly less likely to purchase health insurance and more likely to make out-of-pocket payments for medical care.[23]
Safety-Net Requirements
Early in the twentieth century, hospitals used a combination of charitable donations, public subsidies, and surplus revenues from paying patients to finance the delivery of free and discounted care for the poor.
In 1903, the U.S. Census Bureau characterized 1,493 general hospitals in the U.S. as benevolent institutions—including 220 that were owned by federal, state, and local governments. It estimated that 54% of revenues at private nonprofit facilities came from charges to patients and 11% from public subsidies, with the remaining 35% coming from charitable donations or income from endowments. Public hospitals provided the bulk of free care to the poor, funded largely by local property taxes, with charges to patients covering only 7% of their costs.[24]
Many states exempted charitable private hospitals from local property taxes, with the expectation that they would bear public duties.[25] Hospitals were also excluded from federal income taxation when it was established in 1913, so long as no profits accrued to the benefit of private shareholders or individuals.[26]
In 2021, three-quarters of the community hospitals in the U.S. were exempt from taxation (2,978 as private nonprofit organizations and 944 as publicly owned facilities).[27] A Kaiser Family Foundation study estimated the combined value of the exemption (from federal taxes on corporate income, charitable contributions, and bond interest, along with state and local taxes on sales, income, and property) to be worth $28 billion to nonprofit hospitals in 2020.[28]
In return for the exemption, nonprofit hospitals are subject to “community benefit” requirements, the most important of which is that they must use surplus revenues to provide uncompensated care, improve facilities, train staff, or undertake medical research. This vague provision is enforced at the discretion of the Internal Revenue Service without any specific quantitative requirement, and indigent patients have no right to sue for access to free or discounted care.[29] Indeed, given the complex web of contractual relationships in health care, the IRS finds it hard even to distinguish between for-profit and nonprofit entities.[30] In 2016, even though 30 hospitals provided no community benefit, the IRS had not revoked any hospital’s tax-exempt status in a decade.[31]
The 2010 Affordable Care Act slightly tightened community benefit standards, requiring nonprofit hospitals to publish a formal financial assistance policy, and limited charges and collections from low-income patients.[32] Yet eligibility for discounted or free care is still up to the hospital, and financial assistance policies are typically framed in vague and obscure language, which makes oversight challenging and leaves the IRS unable to enforce terms.[33]
In fact, the blanket exemption of nonprofit hospitals from taxation has inadvertently reduced their incentive to provide charity care because each additional dollar of charity care that they provide yields no additional tax deduction. As a result, for-profit hospitals have tended to dedicate a larger share of their expenditures than nonprofit facilities to charity care.[34] In sum, the tax exemption of nonprofit and publicly owned hospitals serves to reduce the tax burden on hospitals but does not otherwise greatly alter their activities.
The Emergency Medical Treatment and Active Labor Act of 1986 requires Medicare-participating hospitals to screen and stabilize the medical condition of any patient arriving in an emergency room, regardless of ability to pay.[35] But it does not mandate the provision of additional services; nor does it limit the ability of hospitals to charge patients for the care that they provide.
More recently, some states have enacted “fair pricing laws,” imposing specific limits on charges to uninsured patients (Table 1). In California, Minnesota, New Jersey, New York, Illinois, and Rhode Island, such laws protect about 80% of the uninsured, whose expenditures on hospital care have been lowered by an estimated 25%–30% as a result. Fair pricing laws have been associated with reductions in the amount of uncompensated care that hospitals provide but with no increase in mortality, medical errors, or readmissions.[36]
Although California’s Fair Pricing Act does not require hospitals to provide free care to the uninsured, 97% of hospitals did so, and 61% of uninsured hospital visits were eligible for free care in 2011.[37] Overall, the act reduced the average price paid by the state’s uninsured patients from 106% to 32% of Medicare rates.[38]
Table 1
Select State Financial Assistance Mandates and Pricing Regulations for Uninsured
| State | Free Care | Discounted Care | Applies to |
| CA | Income <400%FPL or medical costs >10% income; fees capped at highest rate paid by public payer | All hospitals | |
| CO | Income <250%FPL; may charge only <4% of monthly income for <36 months; fees capped | All hospitals | |
| DE | Income <350%FPL | Hospitals receiving Certificates of Need | |
| GA | Income <125%FPL | Income <200%FPL | Hospitals receiving Disproportionate Share (DSH) |
| IL | Income <200%FPL, with $150 deductible | Income <600%FPL | All hospitals |
| LA | Income <200%FPL, or medical cost >20% of income | Tax-exempt hospitals | |
| MA | Income <150% | Income <300% | All hospitals and community health centers |
| MD | Income <200%FPL | Income <500%FPL; fees fixed | All hospitals |
| ME | Income <150%FPL | All hospitals | |
| NJ | Income <500%FPL; fees capped at 115% of Medicare rates | All hospitals | |
| NY | Income <100%FPL | Income <300%FPL; fees capped at rate paid by highest-volume payer | All hospitals |
| OH | Income <100%FPL | Hospitals receiving state funds | |
| OR | Income <200%FPL | Income <400%FPL | Tax-exempt hospitals |
| RI | Income <100%FPL subject to asset test | Income <300%FPL | All hospitals |
| SC | Income <200%FPL subject to asset test and legal permanent residency | Income <200%FPL | Medicaid-participating inpatient facilities |
| TN | Must limit bills to 175% of cost | All hospitals | |
| TX | Income <21%FPL | Tax-exempt hospitals |
Note: FPL = Federal Poverty Line
In 2019, U.S. hospitals reported delivering $42 billion in uncompensated care, of which $22 billion was free or discounted care for the uninsured, $7 billion was for discounted care for those with insurance, and $14 billion came in the form of uncollected debts among patients with or without insurance.[40]
In 2018, free and discounted care accounted for 1.7% of hospital expenses.[41] But the charity-care burden is not distributed evenly among hospitals: 40% of facilities dedicated less than 1% of expenses to free and discounted care, while 7% of facilities spent over 9% on charity care.[42] On average, U.S. hospitals provided free care to uninsured patients with household incomes less than 179% of the federal poverty level and discounted care to patients with incomes less than 324% of the poverty level.[43] A total of 54% of hospitals restricted eligibility for charity care to local residents.[44]
In the short run, changes in hospitals’ uncompensated care costs reflect shifts in local community needs. A 2015 study found that hospitals’ uncompensated care expenditures rose when the local uninsured population increased, or neighboring hospitals closed. It estimated that each additional uninsured person costs $900 for a hospital.[45]
Compensating Uncompensated Care
The aggregate value of public subsidies to hospitals for providing uncompensated care to the poor is close to the aggregate value of such care that hospitals provide nationwide (Figure 1).[46] But these subsidies are distributed in a way that does not meet the needs of the uninsured.
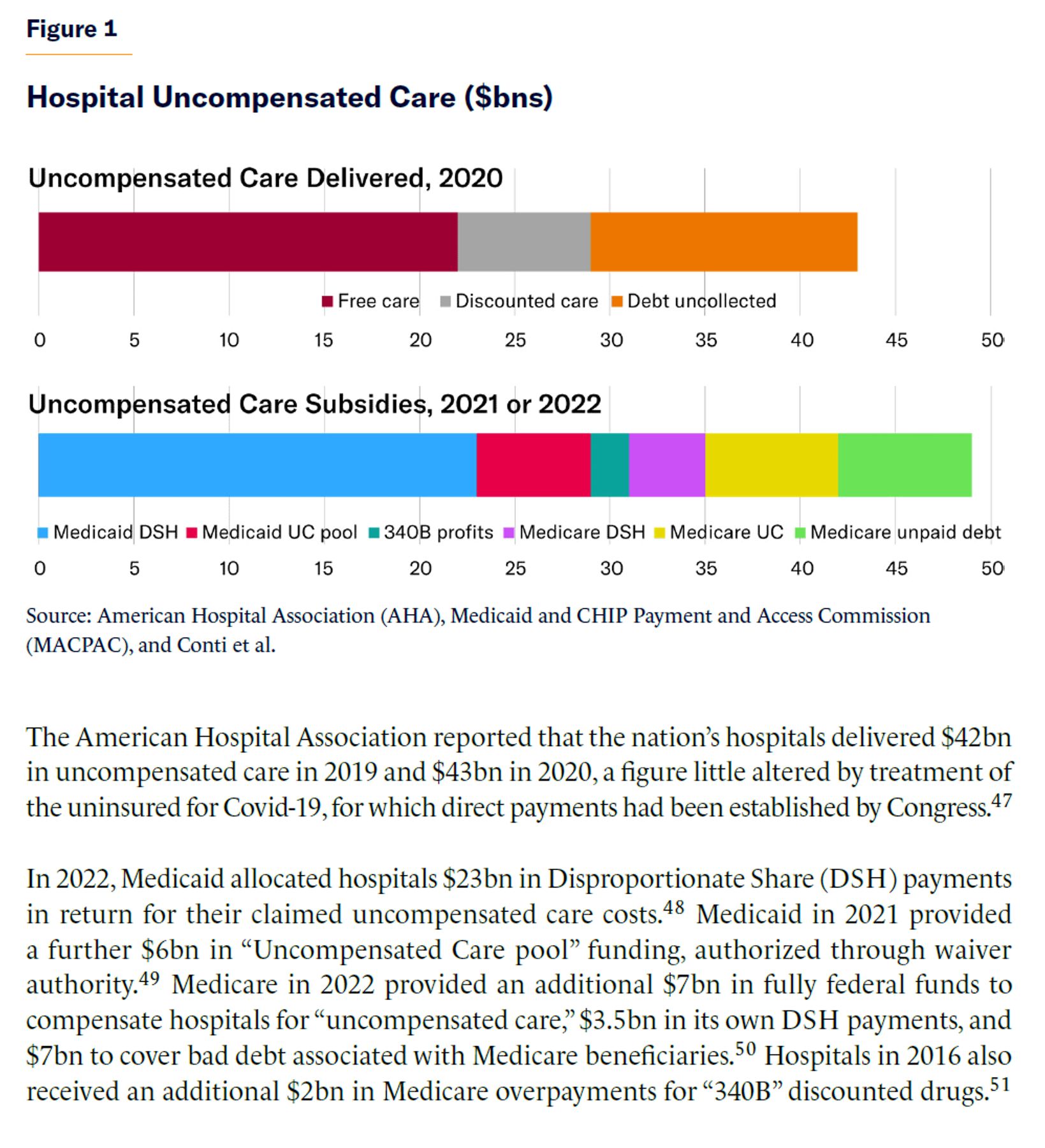
The American Hospital Association reported that the nation’s hospitals delivered $42bn in uncompensated care in 2019 and $43bn in 2020, a figure little altered by treatment of the uninsured for Covid-19, for which direct payments had been established by Congress.[47]
In 2022, Medicaid allocated hospitals $23bn in Disproportionate Share (DSH) payments in return for their claimed uncompensated care costs.[48] Medicaid in 2021 provided a further $6bn in “Uncompensated Care pool” funding, authorized through waiver authority.[49] Medicare in 2022 provided an additional $7bn in fully federal funds to compensate hospitals for “uncompensated care,” $3.5bn in its own DSH payments, and $7bn to cover bad debt associated with Medicare beneficiaries.[50] Hospitals in 2016 also received an additional $2bn in Medicare overpayments for “340B” discounted drugs.[51]
Increased payments for hospital care typically lead facilities to incur higher labor and capital costs when treating patients.[52] In the early 1980s, Congress capped hospital fees for Medicare and Medicaid. But facilities in poor neighborhoods serving mostly Medicaid or uninsured patients struggled to cover their overhead costs through revenues from privately insured patients, so Congress added bonus payments to Medicare and Medicaid for hospitals that treat a “Disproportionate Share” (DSH) of patients without private insurance.[53]
States realized that the absence of a direct link between the ability to obtain Medicaid matching funds and the obligation to deliver services gave them an opportunity to claim a windfall in federal funds. States would artificially inflate Medicaid DSH costs by imposing taxes on hospitals, and then give them kickbacks for participating in the scam.[54] DSH spending surged from $1 billion in 1990 to $17 billion in 1992, before Congress capped the funds that each state could claim. This entrenched an essentially arbitrary distribution of federal aid: in 2023, New Hampshire received $2,123 in Medicaid DSH grants per poor resident; Wyoming, only $4.[55]
Nationwide, Medicaid DSH payments alone amounted to 75% of the cost of “uncompensated” hospital care provided to the uninsured in 2014. But Medicaid DSH payments ranged from 2% of the value of such care provided in Wyoming to 269% in the District of Columbia—exceeding the level of uncompensated care for the uninsured in eight states.[56]
Within states, the distribution of DSH payments is often highly politicized and skewed. In 2014, California and Maine distributed 100% of their Medicaid DSH funds to publicly owned hospitals.[57] States tend to allocate subsidies to hospitals with larger uncompensated care losses, but these subsidies do not expand and contract in line with fluctuations of uncompensated care costs.[58] Many hospitals claimed DSH payments that simply shouldn’t have been allowed under federal law. A 2010 GAO audit found that 717 hospitals received Medicaid DSH payments that exceeded their entire spending on uncompensated care.[59]
States have increasingly sought even more flexibility in distributing subsidies for hospitals to deliver care to the uninsured, by claiming Medicaid DSH funds through a waiver establishing an uncompensated care pool.[60]
The rationale for Medicare DSH funding was similar to that for Medicaid DSH, but the former is distributed as an add-on to Medicare payment rates for inpatient hospital care (ranging up to 19%) at facilities serving large numbers of low-income patients who are eligible for public assistance benefits. As a result, Medicare DSH funds increase with the volume of care provided to Medicare patients and with the share of Medicaid patients, rather than in proportion to the care delivered to the uninsured.
From 1988 to 2020, the share of urban hospitals qualifying for Medicare DSH payments expanded from 35% to 82%. The Affordable Care Act of 2010 sought to improve the distribution of Medicare DSH funds by placing 75% of these funds into a Medicare Uncompensated Care pool. Distribution from the pool is in proportion to a hospital’s share of uncompensated care relative to that provided by all DSH hospitals nationwide.[61] However, this formula does not necessarily reward hospitals for providing discounted care to the uninsured, as opposed to other uncompensated care (such as the forgiveness of unpaid bills by patients who may not be poor). Uncollected medical debt accounts for a third of the uncompensated care provided by hospitals. Yet Medicare reimburses medical providers for 65% of the value of unpaid cost-sharing due from Medicare beneficiaries.[62]
In 1992, Congress created the 340B drug discount program, requiring manufacturers to give DSH hospitals discounts ranging from 25% to 75% on physician-administered drugs—ostensibly, for the purpose of allowing these hospitals to treat patients with little ability to pay.[63] However, Medicare payments for hospitals to purchase these drugs have not been proportionately reduced, leaving hospitals with an annual profit at taxpayers’ expense (growing rapidly in proportion to drug prices and volumes), which they say allows them to fund uncompensated care.[64] There is no legal requirement that hospitals use profits from 340B drug reimbursement to finance uncompensated care.
The nonprofit tax exemption is often criticized as a subsidy but mostly represents the absence of taxes of various magnitudes, which would otherwise arbitrarily inflate the cost of hospital care.[65] (Only the tax deductibility of charitable contributions, worth $2.5 billion in 2020, provides additional revenue to facilities.)[66] The value of the tax exemption is therefore not counted as part of the public subsidy for uncompensated care.
Policy Recommendation: Consolidate Subsidies, Cap Collections
The current patchy system of indirect federal aid to treat the uninsured—which costs taxpayers more than the aid that is provided to those in need—neither allocates funds where they are needed nor protects indigent patients from exorbitant bills. Reforms to the current system would help address these issues without eliminating the responsibility or incentive for Americans to purchase insurance.
Proposal
Federal funds to support the provision of health-care services for the low-income uninsured should be consolidated into monthly capped reimbursement grants for uncompensated care (UC grants).
These grants should be distributed directly to hospitals in proportion to the value of uncompensated free and discounted care (valued at Medicare rates) that they provide to patients with incomes below 300% of the federal poverty rate, up to a cap. Monthly caps on payments to each facility should be proportional to the share of the national uninsured population resident in each hospital’s designated patient catchment area, adjusted by the Medicare Geographic Practice Cost Index. The total amount of federal funds available to support uncompensated hospital care nationwide should automatically adjust every month, depending on the share of the U.S. population that is uninsured.
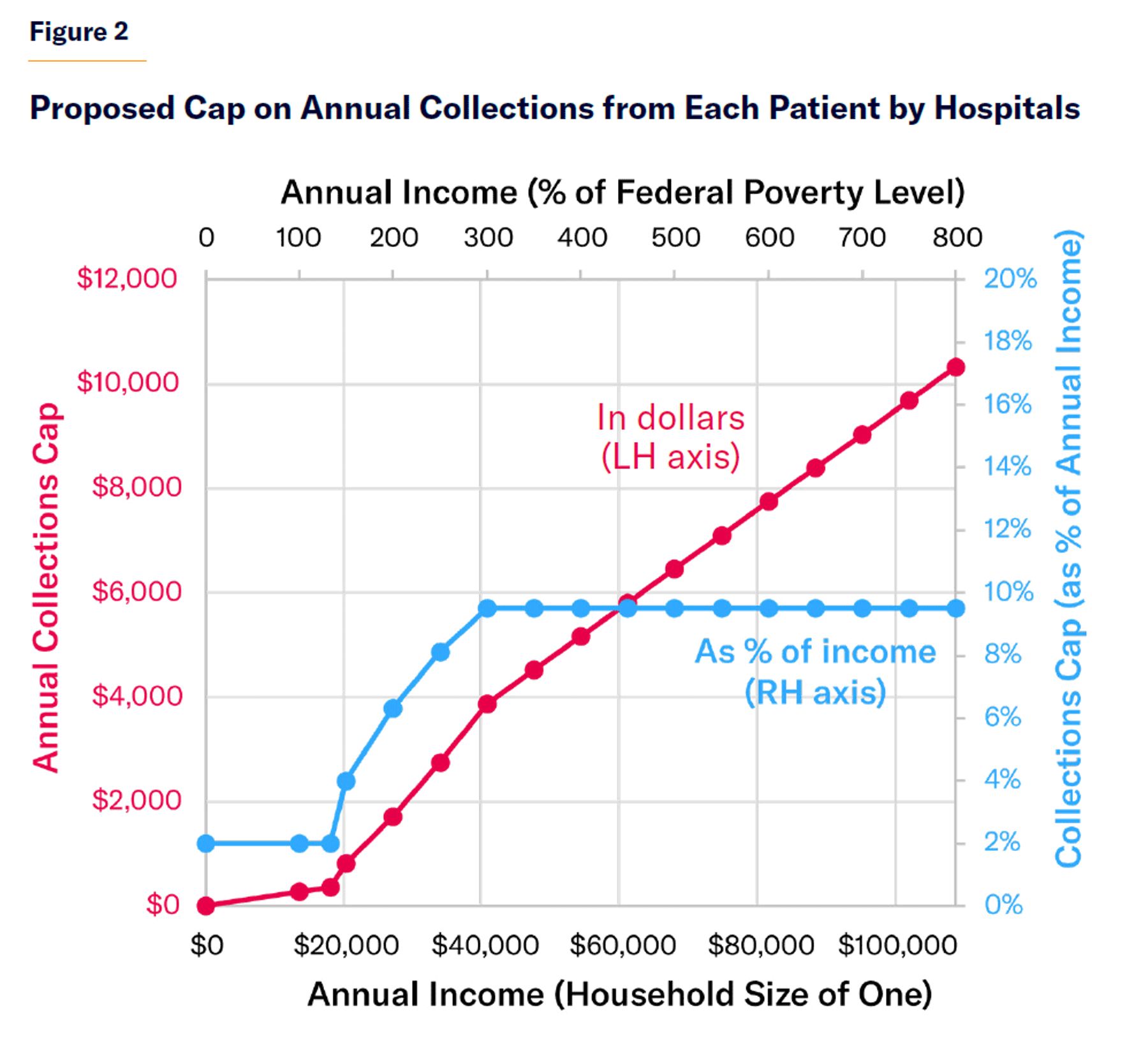
Hospitals and resident providers that accept these grants should be required to cap charges for uninsured low-income patients (with incomes less than three times the federal poverty level) at Medicare rates. The amount of medical debt that hospitals and associated providers may collect every year from uninsured patients should be capped as a percentage of their household income (Figure 2).[67] The IRS should be authorized to certify the income of uninsured patients seeking caps on charges for hospital care that they have received.
Hospitals must still treat and stabilize uninsured patients, as per the current federal Emergency Medical Treatment and Active Labor Act (EMTALA), subject to billing and collection caps. They may also use capped UC grants to finance additional services—again, subject to the proposed caps.
Justification
UC grants would provide several advantages over the current inefficient web of indirect grants, cross-subsidies, regulations, and grants of market power (such as Certificate of Need laws) that are used to finance uncompensated care. UC grants, by contrast, would provide a stable and transparent financing mechanism for hospital safety-net care, and they would improve the distribution of federal aid for uncompensated care, so that it fills the unmet needs of the uninsured, rather than serving to inflate hospital costs in affluent neighborhoods.
UC grants would strengthen the basic safety net of care for uninsured patients and clarify hospitals’ obligations to deliver free and discounted care to them. In addition, they would regularize the existing jumble of federal aid to support uncompensated care, so that it is distributed where it is most needed, without encouraging Americans to drop insurance coverage and without increasing the burden on taxpayers.
Although hospitals would be allowed to claim reimbursement only for uncompensated care provided to patients with incomes below 300% of the poverty level, caps on charges would apply to all uninsured patients, in all states, at for-profit, nonprofit, and public hospitals alike. Caps on billing and collections would reduce disputes arising from uncertain patient liability for care, while eliminating the most heavy-handed and futile attempts to collect repayment.
The aggregate cap on UC grants would encourage hospitals to reserve federal aid for the treatment of patients who lack good insurance coverage or the ability to pay for care. Meanwhile, limiting UC reimbursement claims to Medicare rates would ensure that facilities are providing appropriate amounts of uncompensated care in return for the federal aid that they claim, without merely inflating fees. Because reimbursement grants would be based only on uncompensated care for patients below 300% of FPL, and charges that are collected would be deducted from a hospital’s UC grant, hospitals would be gently nudged to concentrate UC grant funds on lower-income uninsured patients.
Providing clear income-based caps on charges, certified by the IRS, would permit a more accurate assessment of uninsured patients’ income, while reducing the harassment of indigent patients. Relative to current practice, this would yield a more graduated distribution of discounted care according to income.[68] By helping hospitals assess the ability of uninsured patients to pay for care, it would also increase the incentive for those with higher incomes to purchase insurance.
Patients would be protected by repayment schedules but not guaranteed an entitlement to any defined set of free or discounted medical services, beyond those currently defined under EMTALA. Although this reform would protect low-income patients from exorbitant changes, it would not eliminate the incentive to purchase insurance or enroll in entitlements to gain access to prescheduled elective medical services. Annual income-contingent repayment requirements would be similar to income-contingent subsidized insurance premiums on the exchanges established by the Affordable Care Act; but the latter would confer access to a much wider set of health-care services.
The combination of UC grants and caps on collections from uninsured patients would leave hospitals with flexibility to meet their local communities’ uncompensated care needs. The absence of rigid rules for the distribution of federal aid among individual patients would allow hospitals to set their own policies regarding eligibility for free and discounted services and the intensity of medical care provided on a free and discounted basis. The flexibility regarding eligibility for free and discounted care would facilitate the resolution of politically challenging uncompensated care challenges, such as the degree to which federal funds can be used to subsidize the care of noncitizens.
Endnotes
Photo: JazzIRT/iStock
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).