Deinstitutionalization Redux The Decline in Residential Mental Health Treatment for Youth

Photo: Imgorthand/E+ via Getty Images
Executive Summary
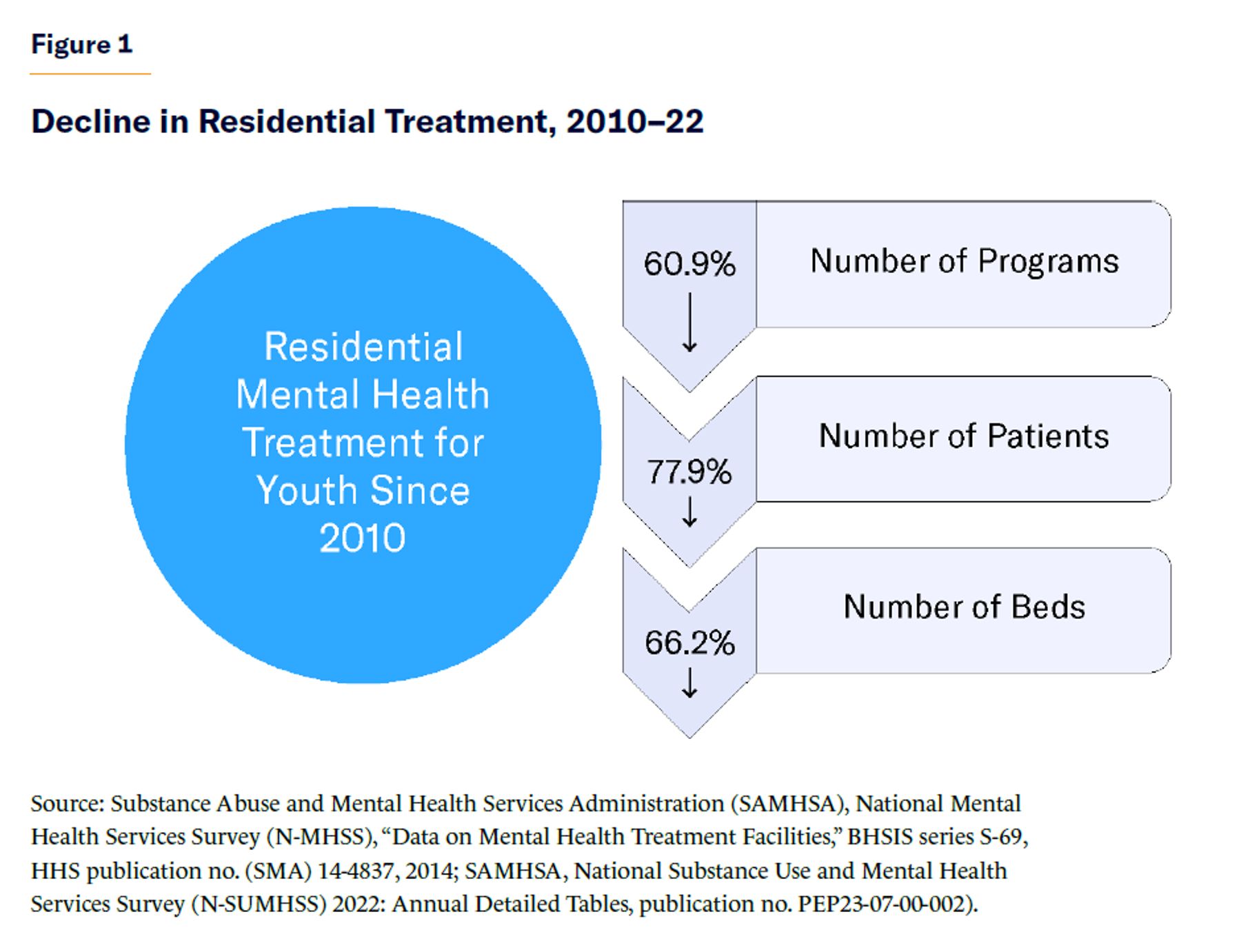
In recent years, there has been much debate about how to address the high and growing rates of mental health issues facing American youth. But at the same time, one potential solution—youth residential mental health treatment—has sharply declined in availability. Less intensive than hospitalization, but more so than outpatient services, residential programs are a critical component of the youth mental health-care continuum. By all measures—e.g., number of programs, beds, utilization—youth residential treatment has been declining (Figure 1), even as a range of adverse outcomes in youth mental health have been spiking. The declines have been driven not by evidence of failure but by ideological opposition to this mode of treatment.
This report surveys the youth residential mental health treatment landscape, documents its recent decline, and explains the reasons for the decline. It highlights the clinical benefits of residential treatment programs and makes recommendations for stabilizing their supply and expanding access.
Chief findings include:
- Since 2010, the number of youth residential mental health treatment programs has declined by 60.9%, the number of youths served has declined by 77.9%, and the number of beds has declined by 66.2%.[1] The number of beds available in youth residential treatment programs has declined faster than did available psychiatric hospital beds during the era of deinstitutionalization of the mentally ill.
- These decreases coincide with (for youths) high and rising rates of suicide, usage of psychiatric hospitals, emergency department (ED) boarding, and criminal justice involvement.
- Notwithstanding advocacy and media criticisms of isolated tragedies, on-site surveys of residential treatment facilities show that they are as safe as general hospitals.
Despite these alarming trends, advocates and policymakers continue to pursue reductions. With rhetoric echoing the most radical proponents of deinstitutionalization, they have advocated for the elimination of youth residential treatment. This harmful ideological approach should be avoided in favor of improving and expanding high-quality residential treatment. To that end, this report recommends:
- Exempting residential treatment programs from the Institution for Mental Diseases (IMD) exclusion
- Expanding the use of §1115 Medicaid waivers
- Increasing the youth behavioral health-care workforce
- Improving timely access to other levels of behavioral health care, including inpatient
- Ensuring that funds—particularly for education—follow children to their place of treatment
Introduction
Mental health care for children exists on a continuum. At the low end is early intervention; at the high end is inpatient hospital care, which is the most clinically intensive and restrictive option and is typically reserved for children in an emergency. One step below this is residential treatment, which is nonhospital inpatient care that is often recommended for children with previously unsuccessful experiences at lower levels of care. Patients in residential settings are often considered difficult to treat because of their behavior, acuity, and clinical complexity (Figure 2).
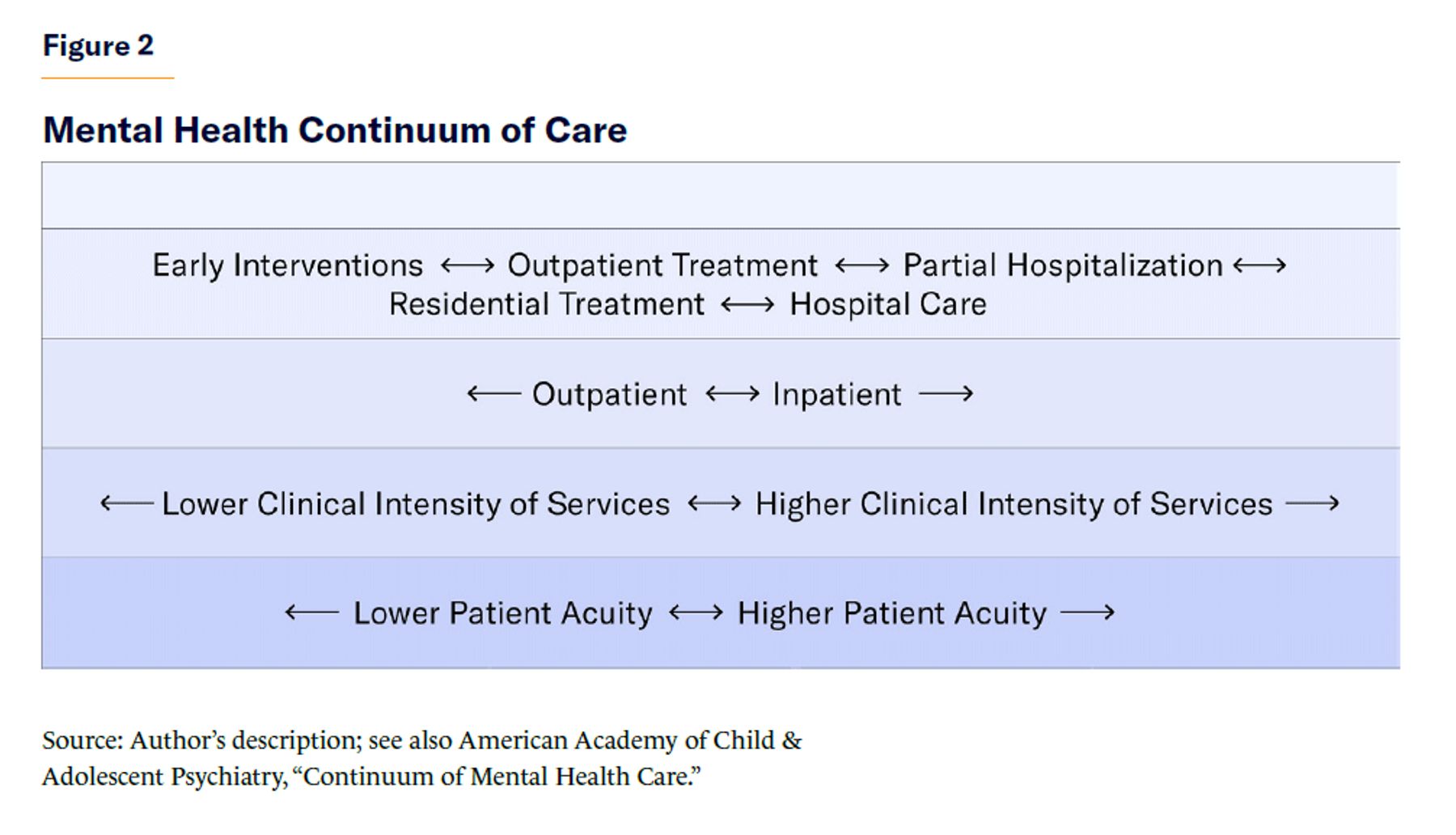
A child’s mental health treatment placement is not typically determined by the child but by a parent, caregiver, or—in the case of some children in foster care—the state. Parents, caregivers, and states never desire residential treatment as the first treatment option for children. It becomes necessary only when a child’s clinical acuity reaches a level where his or her well-being depends on it. The American Academy of Child and Adolescent Psychiatry states: “Residential treatment can help children and adolescents whose health is at risk while living in their community. For example, the programs are helpful for those who have not responded to outpatient treatments, who have education needs that cannot be met in less restrictive settings at their local schools, or who are in need of further intensive treatment following inpatient psychiatric care.”[2]
Wilderness programs, boot camps, military schools, and specialized boarding schools for troubled youths are residential programs, but they do not have a clinical focus and thus are not “mental health” treatment programs. Residential mental health treatment programs for youth are staffed by multidisciplinary teams of licensed professionals including psychiatrists, psychologists, social workers, nurses, and special-education teachers. These teams provide a variety of services and supports to meet the psychiatric, social, and educational needs of children.
For purposes of this report, a residential treatment program means a Psychiatric Residential Treatment Facility (PRTF) or a Qualified Residential Treatment Program (QRTP).[3] PRTFs are one of three specific settings—the others being psychiatric hospitals and psychiatric units of general hospitals—that are permitted to receive reimbursement under Medicaid’s Psych Under-21 benefit, which allows these institutions to provide inpatient psychiatric services for enrollees under age 21[4] that would otherwise be prohibited by the Institution for Mental Diseases (IMD) exclusion.[5] The Joint Commission, Council on Accreditation (COA), Commission on Accreditation of Rehabilitation Facilities (CARF), or a state-approved accrediting organization is responsible for accrediting PRTFs. In addition to any state laws, a PRTF must meet federal standards for certification and comply with the federal Conditions of Participation (COP). Federal law also requires that they deliver care under the direction of a physician in a safe and appropriate environment and in the least restrictive manner possible. Each patient must have an individual plan of care that states the treatment objectives, prescribed interventions, and post-discharge plans.
Not every state has a PRTF. In 2023, only 34 states had at least one PRTF. If a state chooses not to have a PRTF, it is still responsible for providing those services to all enrollees who need them. To meet this requirement, a significant number of children are sent from their home state to states with a PRTF.
In 2018, for the first time in federal law, the Family First Prevention Services Act (FFPSA) defined a QRTP.[6] QRTPs focus on foster children and provide less clinically intensive care than PRTFs. As defined by FFPSA, QRTPs must be accredited by the Joint Commission, COA, CARF, or a state-approved accrediting organization.[7] They have to be able to provide trauma-informed treatment models to children with serious emotional disturbances and continuously have registered or licensed nursing staff available.
Because QRTPs are not exempt from the IMD exclusion, they cannot bill inpatient Medicaid rates. Instead, children in QRTPs receive federal title IV-E foster-care maintenance payments for room and board and Medicaid outpatient payments for clinical services. FFPSA mandated that non-PRTF residential facilities meet a complex series of new clinical and reporting requirements to keep receiving title IV-E funding—but the bill provided no additional funding to meet these new requirements.
PRTFs and QRTPs differ in three ways: (1) PRTFs provide more clinically intensive services to higher-acuity children than QRTPs; (2) PRTFs care for children generally, whereas QRTPs focus on foster children; and (3) PRTFs receive reimbursement as inpatient providers, which covers health-care costs and room and board, whereas QRTPs, because of the IMD exclusion, rely on lower outpatient Medicaid rates and federal title IV-E funding for room and board.
Decline in Residential Mental Health Care for Youth
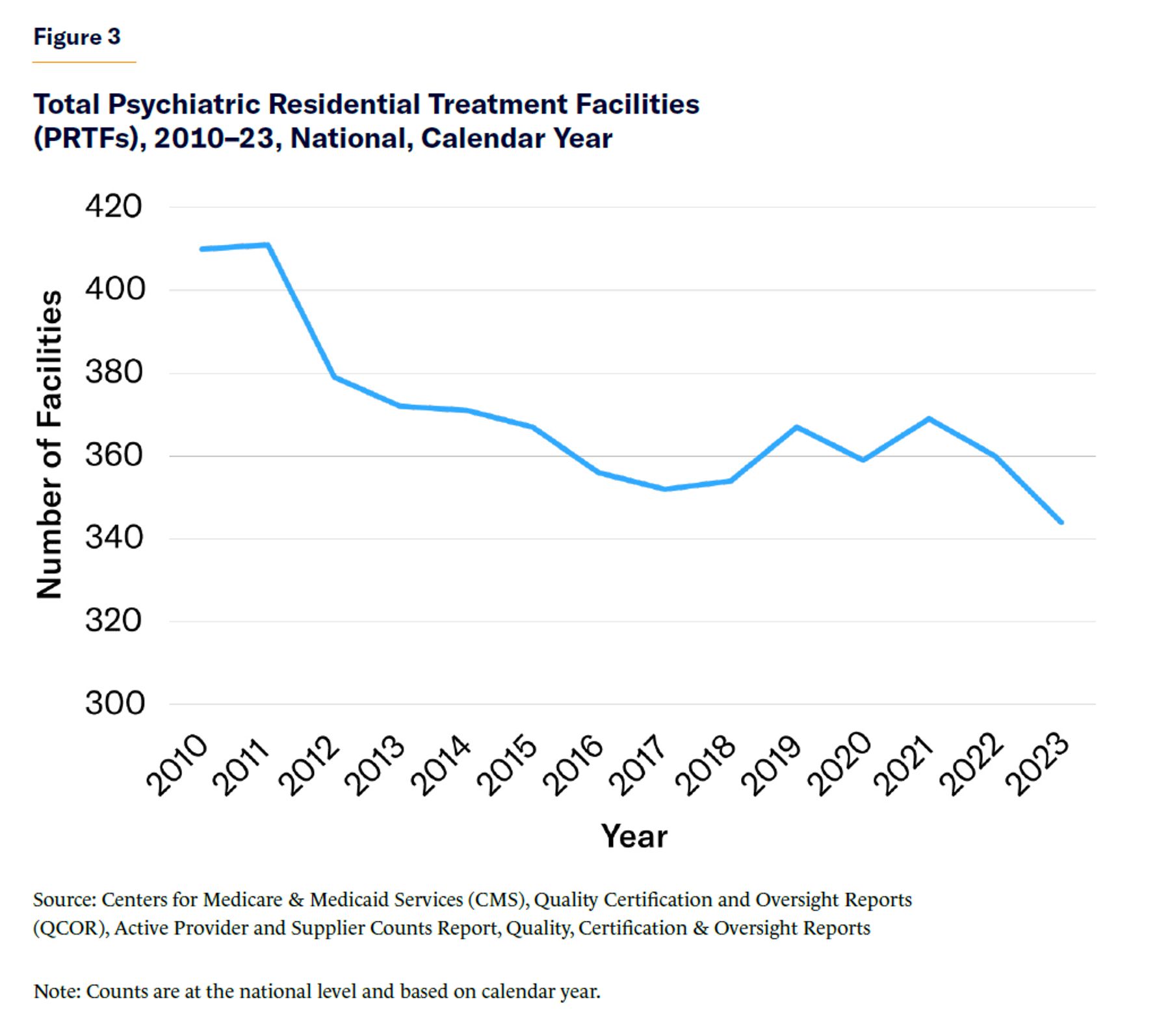
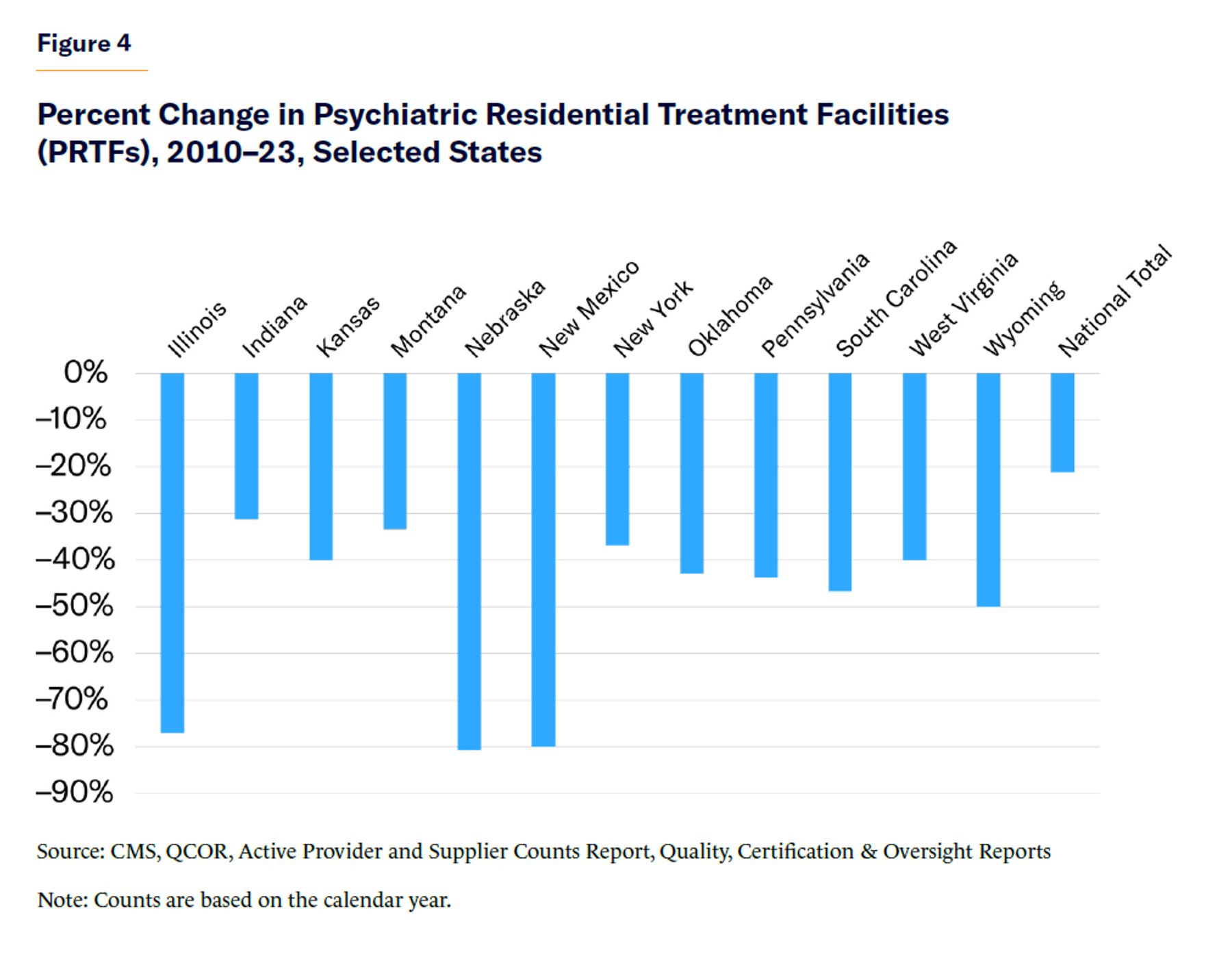
Data from the Centers for Medicare and Medicaid Services (CMS) and Substance Abuse and Mental Health Services Administration (SAMHSA) during 2010–23 show a decline in the number of PRTFs and QRTPs, the number of residential beds, and the number of children served. Total PRTFs have declined from more than 400 in 2010 to fewer than 350 in 2023 (Figure 3). In total, the number of PRTFs has declined by 21% since 2010, and 12 states have experienced declines of over 30% (Figure 4).[8]
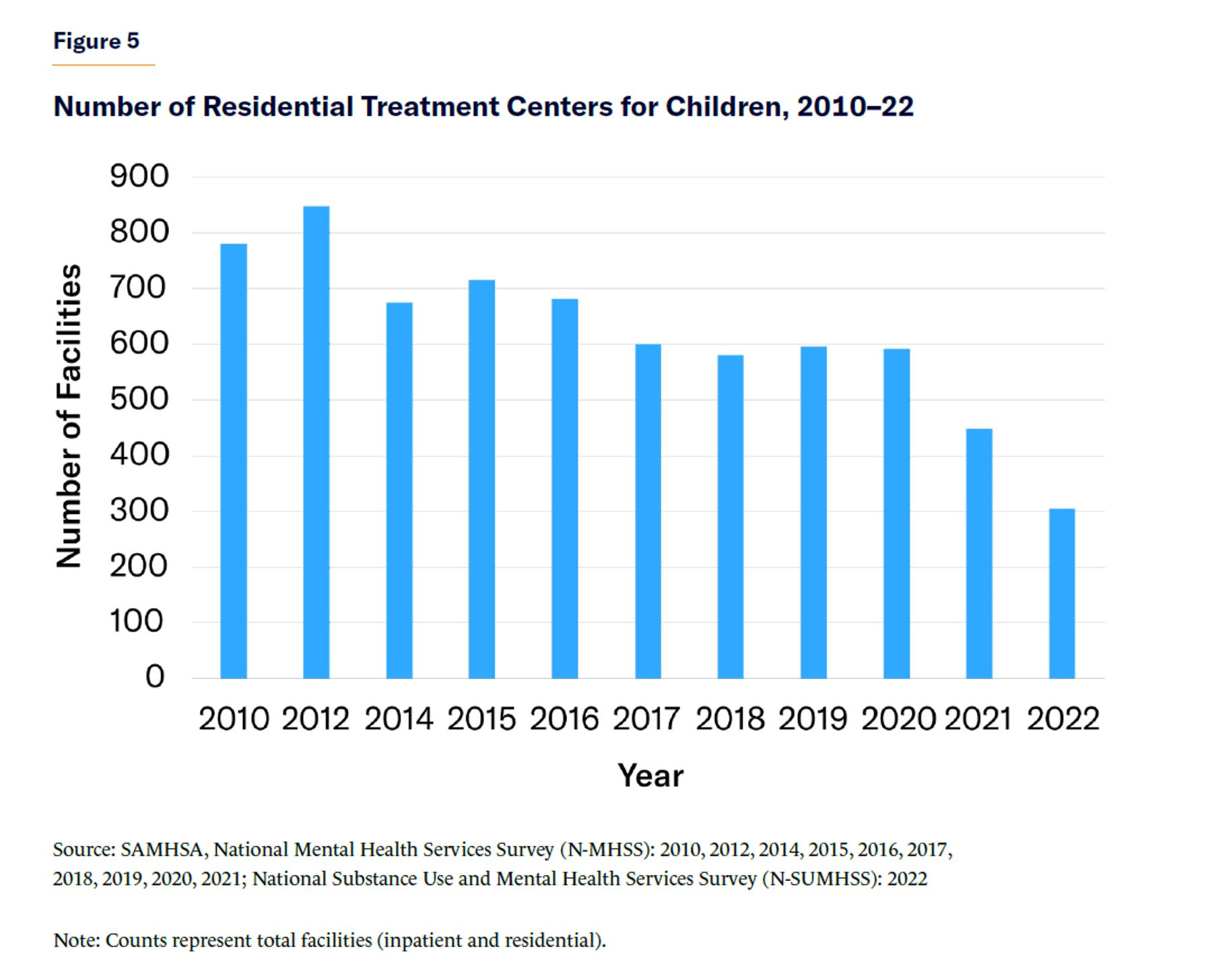
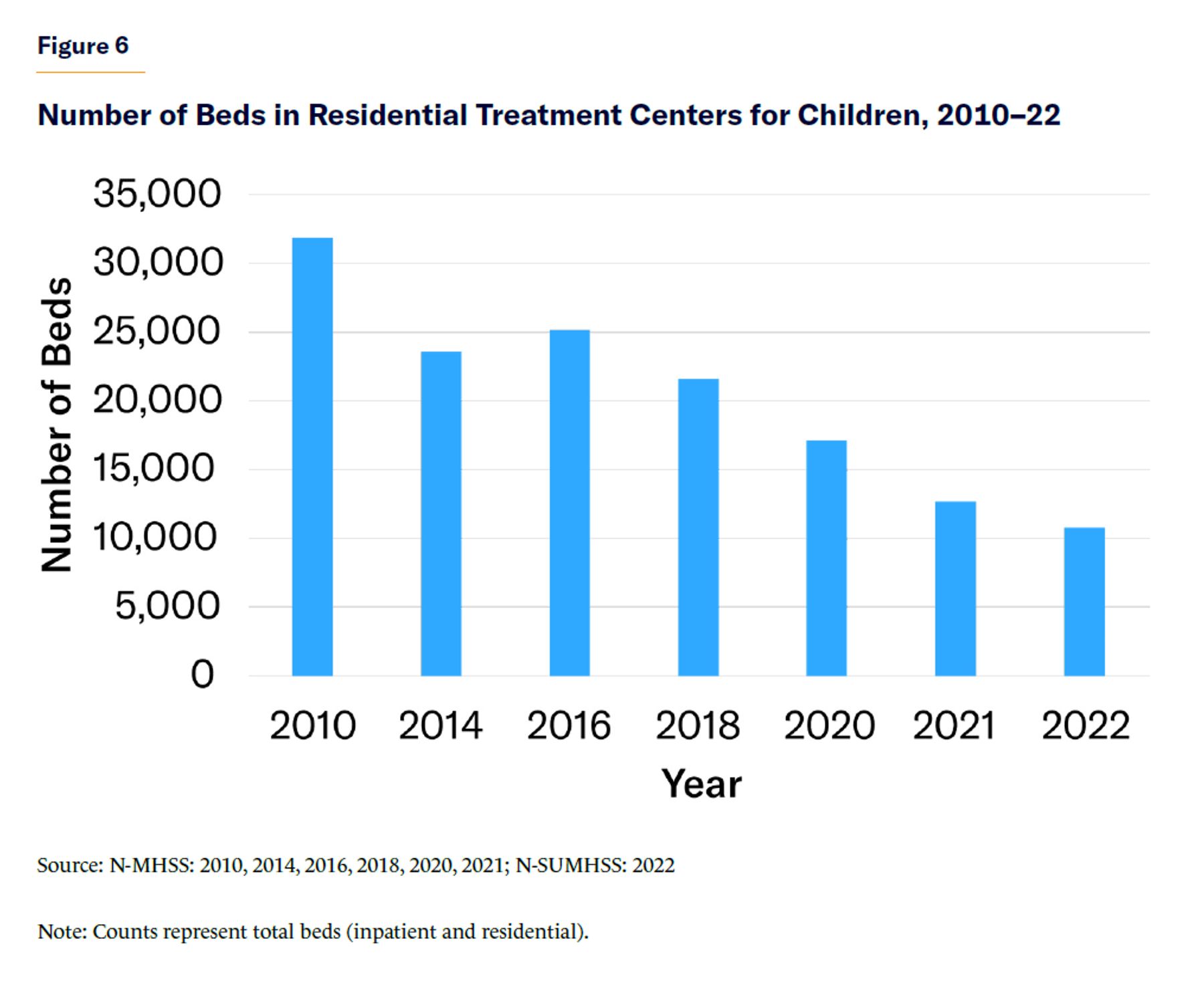
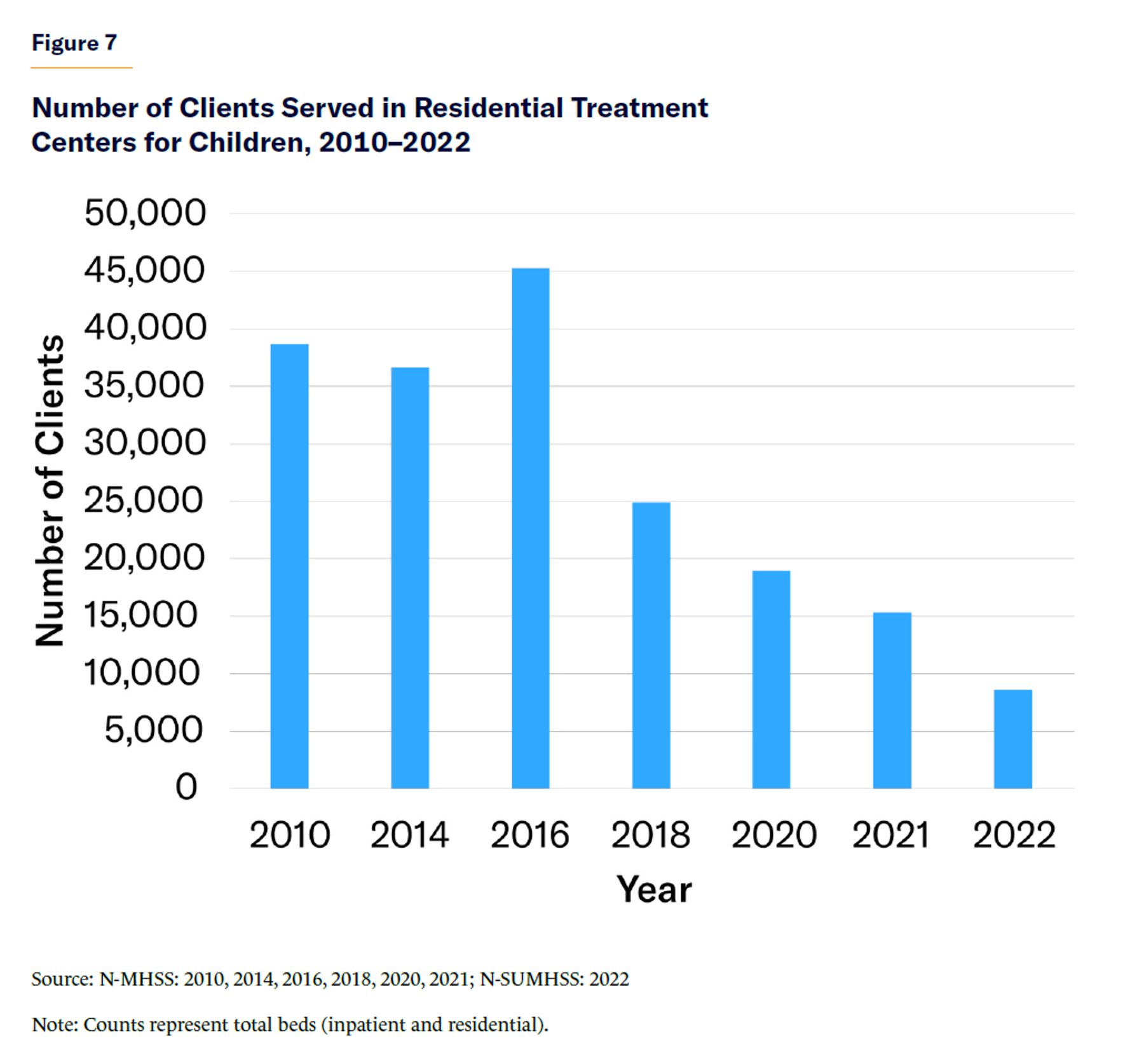
Every two years, SAMHSA also releases data on the number of beds and the number of patients served in “residential treatment centers (RTCs) for children,” which include QRTPs. Since 2010, the number of such facilities has declined 60.9% (Figure 5), and the number of beds has declined 66.2% (Figure 6).[9] The number of beds has declined by almost half, just since the passage of FFPSA in 2018. The number of children served in RTCs has declined faster (77.9%) than the number of facilities or the number of beds (Figure 7).[10]
The lack of available beds has made it challenging for states to meet demand. A 2022 report found that “statewide, Texas is meeting under 10% of local demand” for residential treatment; in one region, the state lost 437 beds when a single facility closed.[11] A recent Government Accountability Office (GAO) report found that “in addition to the lack of inpatient beds, representatives from many of the stakeholder organizations we interviewed, including those representing consumers, providers, state health agencies, and an insurance regulator indicated that a shortage of intermediate care options such as residential treatment facilities or intensive outpatient programs has created challenges for consumers in getting intermediate levels of care.”[12]
Some states have responded by sending children out of state for residential treatment.[13] A report based on data from the Administration for Children and Families found that 1,716 children were sent out of state for residential treatment in 2018.[14] However, in response to abuses at some out-of-state programs to which youths had been sent, California banned out-of-state placements for foster youth and juvenile offenders in 2021.[15] These challenges will likely become only more acute as FFPSA is fully implemented and the new requirements take effect.
Three Waves of Youth Residential Deinstitutionalization
These declines are not an accident. They are the result of deliberate policies advanced by advocates and implemented by policymakers who believe that youth residential treatment is overused and dangerous. According to one advocacy group, there is an urgent need for a “reduction of residential care utilization and associated costs” because residential care should be used only “as a last resort” and “any amount of time that a young person spends in an institutional placement is too long.”[16] Another advocacy group summed up this philosophy in a 2021 report, which described youth residential treatment as “insidious” and proposed a goal of reducing all residential placements to zero.[17]
Ideological opposition to youth residential treatment is not new—rather, it is part of a 30-year trend that has unfolded in three waves. The first wave of policy changes occurred in the 1990s and focused on “extensive gatekeeping procedures” to redirect children away from residential treatment.[18] The intent was to make residential treatment the last resort by funneling children to any other service provider. One report on these “gatekeeping procedures” implemented in Illinois in the mid-1990s found that they “produced their desired effect”—residential utilization “declined consistently and dramatically” at a “much faster rate than utilization of all other types of placements.”[19]
The second wave occurred in the 2010s, when the federal government started enforcing stepped regulations on PRTFs in new and onerous ways. CMS finalized its PRTF regulations in 2001, when states began to offer these services, but enforcement was not draconian at first. By 2010, however, CMS had begun zealously enforcing the technical components of the regulations, which made it difficult for states to comply. Minnesota, for example, had been providing PRTF services for several years when CMS informed the state that its programs did not meet the requirements and would no longer be exempt from the IMD exclusion. This meant that the state’s PRTFs could no longer receive inpatient reimbursement—and for many programs, the outpatient rates were simply not sustainable. The Children’s Intensive Mental Health Services Study, commissioned by the Minnesota Department of Human Services, states: “In 2018 … CMS made a final decision to define many of Minnesota’s current children’s residential treatment facilities as Institutes of Mental Disease (IMDs)—and therefore ineligible to receive federal Medicaid reimbursement for treatment services…. [T]he state had actively opposed these facilities being classified as IMDs, and the state’s rationale was accepted by CMS for a number of years.”[20]
The third wave came with the passage of FFPSA in 2018.[21] FFPSA was premised on the idea that any stay at a residential program is too long; it thus erroneously used the length of stay as a proxy for quality. FFPSA required residential programs, on a near-constant basis, to demonstrate that a patient is appropriate for residential care to a third party. Each child in a QRTP must have an evaluation within 30 days of placement by a “qualified individual” to determine whether another appropriate placement can meet the child’s needs, among other criteria. The qualified individual must file this assessment with the district court within 35 days of placement. Within 60 days of placement, the court must issue an order approving or disapproving the placement. This documentation on appropriate placement must continue to be demonstrated at each status review. Then, after 12 consecutive months or 18 nonconsecutive months, the head of the state child-welfare agency must submit an approval for continued placement to the secretary of Health and Human Services. This rigorous and demanding review process was explicitly designed to limit the length of stay at QRTPs.
Little evidence supports the notion that shorter stays in residential treatment are beneficial to children with serious emotional disturbances; indeed, some evidence indicates the opposite. One of the “most extensive studies ever conducted of residential care” found that “having been in residential care for less than 90 days significantly increased the likelihood of stepping back up to residential placement.”[22] The study attributed this, in part, to the fact that for “some youth with considerable instability in their lives, stays of 90 days or more may be needed to help them build a sense of trust and security in their relationships with adults and in their own capacities.”[23] Another study associated stays of shorter than 90 days with increased readmissions, and 45% of those readmissions occurred within 21 days after discharge.[24] These researchers noted that the “results of this study supported both of our hypotheses that length of stay and severity of functioning at discharge predicted recidivism at a children’s RTC.”[25] And the “findings of this study in combination with previous studies suggest that there may be a subset of children and adolescents (26%) whose shorter lengths of stay in residential treatment are increasing their risk of future readmissions.”[26]
Challenges in Youth Mental Health and the Decline in Residential Treatment
While the availability of youth residential treatment programs has been declining, there has been a simultaneous increase in adverse mental health outcomes among youth.
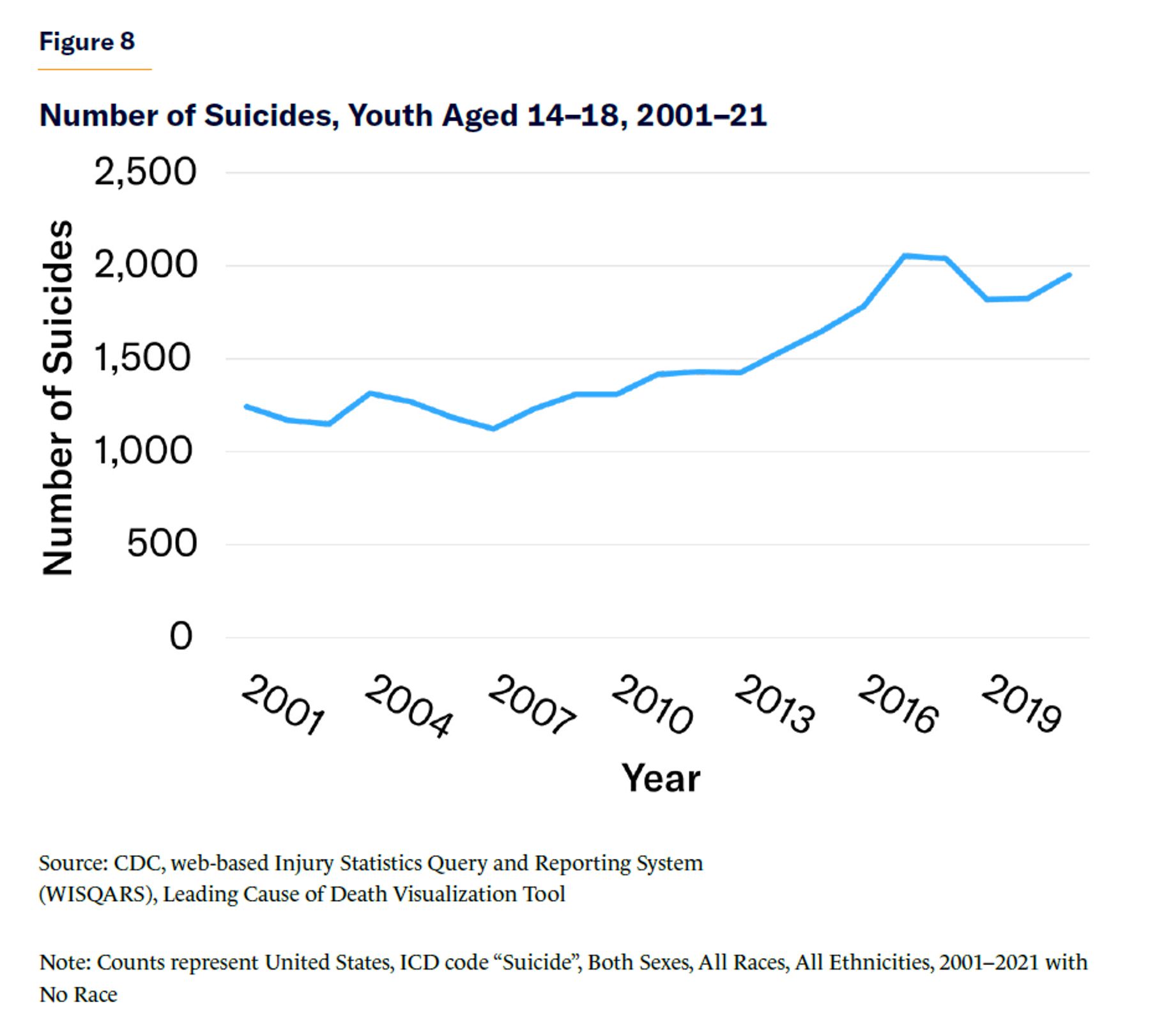
Suicidal ideation and suicide attempts are among the most common reasons that a youth requires residential treatment. As access to residential treatment has declined, suicide deaths among the 14–18 cohort—the target age range for residential treatment programs—have increased (Figure 8).[27]
More generally, suicides for all individuals under 18 have increased by close to 50% over the past decade.[28] In 2021, suicide was the third leading cause of death among youth (18 and younger), trailing unintentional injury and homicide.[29]
Over the same period, there has been an increase in utilization of inpatient services for youth with mental health conditions. A study published in March 2023 found that, while the total number of pediatric hospitalizations decreased between 2009 and 2019, the number of mental health hospitalizations increased by an estimated 25.8% for children and adolescents aged three to 17 years.[30] Hospitalization for psychiatric disorders accounts for approximately one-third of all hospital days among youth and adolescents, and psychiatric disorders are the leading reason for hospitalization among Americans five to 19 years old.[31] Youth aged 14–18 visit emergency departments for suicidal ideation at a higher rate than any other age cohort.[32] One review found that, in 2019, the “most common reason for inpatient stays among children aged 10 years and older was depressive disorders” and that “trauma- and stressor-related disorders, suicidal ideation/ attempt/intentional self-harm, and other specified and unspecified mood disorders also were among the 10 most common diagnoses for children aged 10 years and older” with inpatient stays.[33]
Some youth who are seeking inpatient treatment end up “boarded” in EDs, waiting days for care because of limited access to residential treatment.[34] The aforementioned GAO report noted that “officials from one state health agency indicated their state has limited capacity to provide residential treatment, and this issue was particularly challenging for children needing such services. As a result, officials said they frequently hear instances of children being stuck in an emergency room at a hospital, unable to access the care they need.”[35] A concerning new trend among this subset of patients is “atypical boarding,” where a child is abandoned in the ED by parents who can no longer provide for their increasingly aggressive, ill, and troubled child and have no other options.[36]
Up to 70% of juvenile offenders have a mental illness,[37] including 20%–25% with a “severe” disorder.[38] In some juvenile correctional programs, it is estimated that virtually all youths have diagnosable mental disorders.[39] Criminal justice agencies have, for many years, been responsible for large numbers of mentally disordered youth.[40] But the problem may be worsening: according to one study, the portion of youth entering the juvenile justice system in Washington State who were classified as “high risk” for mental health issues increased by 24% during 2011–15.[41]
Existing research is not sufficient to definitively conclude that these increases in adverse outcomes were caused by declines in residential treatment programs; certainly, a host of other factors are at play. But clearly, many children experiencing these outcomes would be better off in a residential treatment program.
Ironically, the push to deinstitutionalize youths by keeping them out of residential programs is leading to more institutionalization—but in psychiatric hospitals and juvenile detention facilities. Historically, residential treatment facilities would have diverted a portion of these patients away from these more restrictive settings. But for many children, that safety valve is no longer available. In some states, both alternatives to juvenile detention—residential treatment and youth beds in psychiatric hospitals—have been declining sharply. New York, for example, has cut almost one-third of its state psychiatric hospital beds for children since 2014; and during 2010–22, it cut more than half its residential treatment beds, from 554 to 274.[42]
The remaining residential treatment programs are increasingly strained. Residential programs are now treating higher-acuity patients with more complex treatment needs with fewer financial resources. A greater portion of the youth in these programs have already gone through failed placements elsewhere or are “stepping down” from more restrictive settings. A 2004 study of facilities in Illinois conducted over nine years—and which coincided with the closure of 60 residential treatment programs in the state—found that the changing caseload was responsible for an increase in negative discharge outcomes (defined as “a psychiatric hospital, detention, running away, or another residential placement”).[43]
Residential Treatment Quality and Outcomes
Youth in high-quality residential treatment programs experience fewer problems and fewer negative behaviors; and those with more serious problems show greater improvement.[44] Residential treatment also improves outcomes for youth with anxiety,[45] obsessive-compulsive disorder,[46] and trauma.[47] Despite the evidence of efficacy, three arguments have been used to justify efforts to reduce or eliminate access: 1) children are unsafe in the residential setting; 2) children who do not need to be in residential care are sent there; and 3) lengths of stay in residential treatment are too long. Anecdotal evidence exists for these arguments, but federal data refute each claim and make clear that residential treatment facilities are as safe as general hospitals, patients in residential treatment clinically need to be there, and longer stays in residential treatment—particularly for seriously ill patients—provide better outcomes.
Safety
Journalistic accounts have raised serious concerns about the safety and mistreatment of patients in some youth residential programs.[48] Instances of patients hurt in the care of a provider are alarming, and every case of abuse or neglect needs to be investigated immediately and punished appropriately. But isolated incidents do not prove a systemic problem or justify reductions in services.
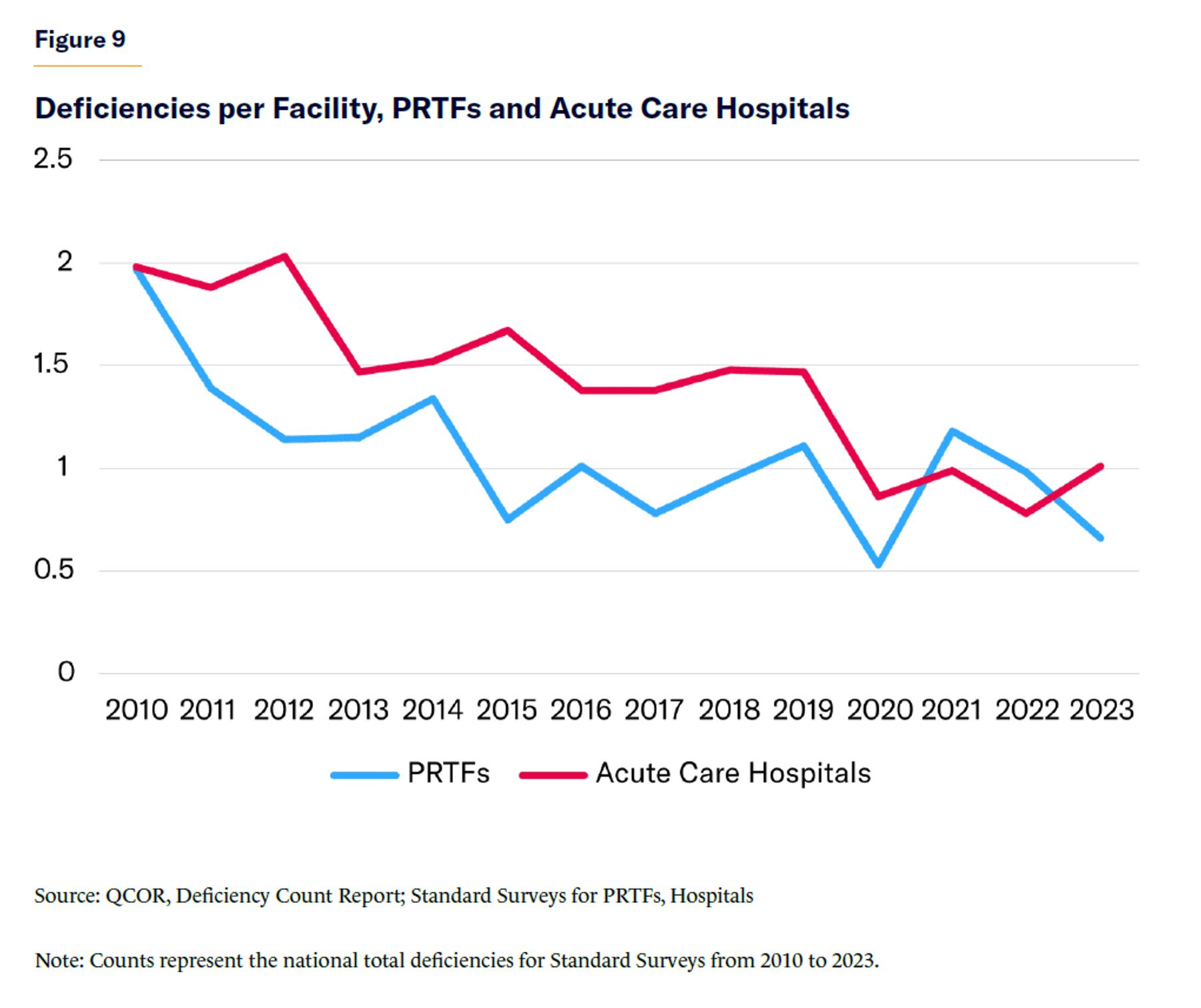
PRTFs, under federal regulation, are subject to rigorous quality and safety specifications and, as a result, are statistically as safe as general hospitals.[49] In 2001, CMS finalized its rulemaking establishing COP for PRTFs and regulating their safety. These COPs include requirements on the use of restraint or seclusion,[50] certifying the need for services,[51] demonstrating active treatment,[52] developing individual plans of care,[53] and the use of interdisciplinary teams.[54] Specifically, CMS’s State Operations Manual Appendix N-Psychiatric Residential Treatment Facilities, updated in 2015, provides 45 pages of Interpretive Guidance for the enforcement of the PRTF COPs.[55] These safety requirements are monitored and audited by independent surveyors from state agencies and nationally recognized accreditation organizations. Data generated from these COP enforcement surveys can be reviewed to see trends in safety and quality in residential facilities.
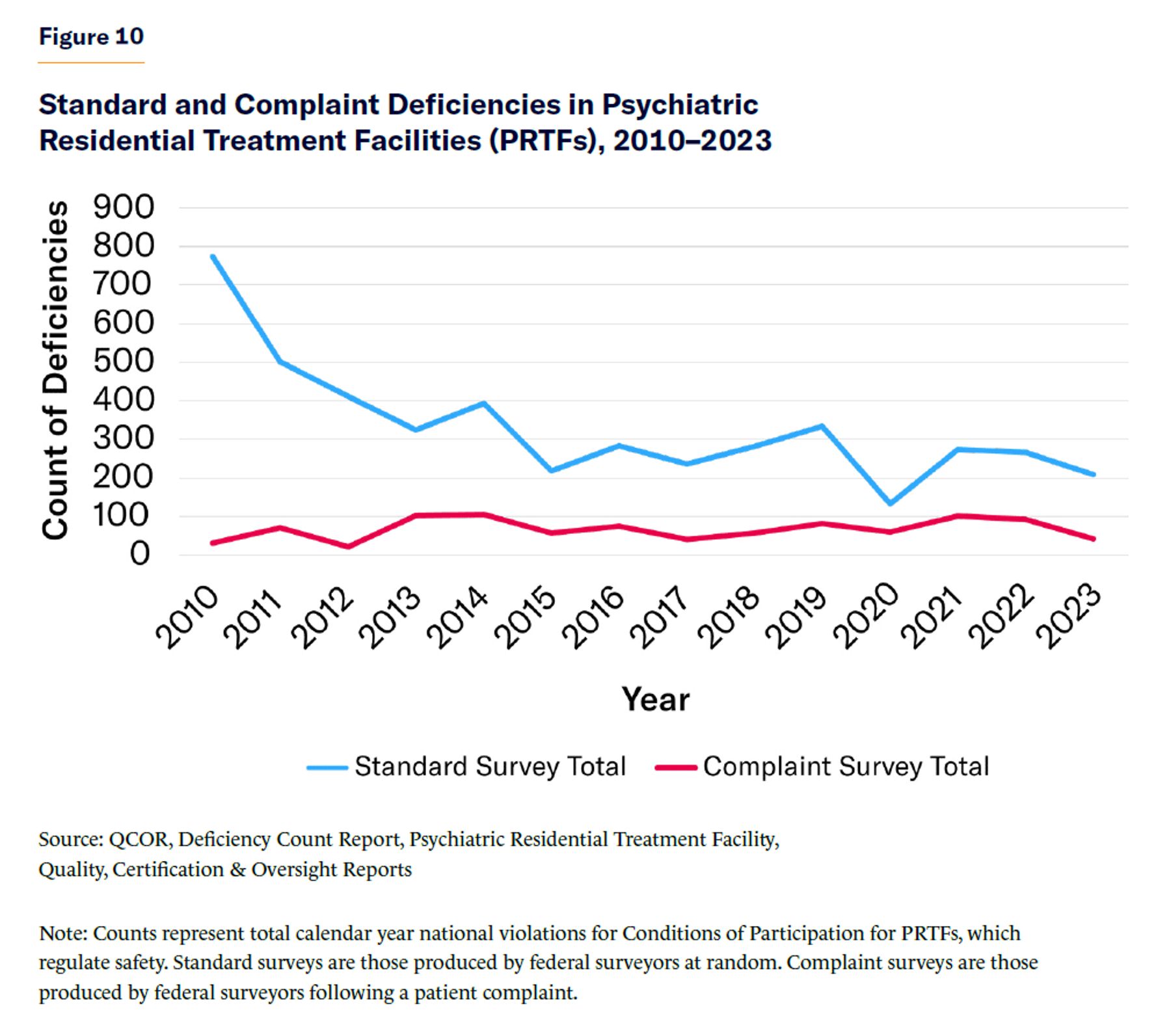
The COPs for PRTFs are different from the COPs for general hospitals, but both serve as safety standards for their respective settings and are reviewed in the same manner. All federal COPs are reviewed: 1) at random by surveyors or standard surveys; and 2) by surveyors following a patient complaint or complaint surveys. The results of these surveys are reported to CMS and published in aggregate on CMS’s Quality Certification and Oversight Reports (QCOR) website.[56] The QCOR data for PRTFs shows that deficiencies (violations of the COPs) on complaint-related surveys and random surveys are on par with those for general hospitals, meaning that PRTFs and general hospitals are, in aggregate, equally as safe (Figure 9).[57] Additionally, the number of standard deficiencies in standard surveys has been declining, indicating that PRTFs are getting safer over time (Figure 10).
Lengths of Stay
Critics of youth residential treatment facilities often claim that youths are kept in these settings for too long. But they overlook the myriad existing controls on access to residential treatment and lengths of stay, such as utilization review, which guard against overly long stays, and may unnecessarily shorten them.
Clinical settings like QRTPs and PRTFs are subject to rigorous and individualized utilization review processes that require them to justify to payers the care that they provide. These reviews, designed to safeguard against overutilization, are so restrictive that they have been criticized for violating federal mental health parity laws.[58] A February 2023 report from Vermont shows how these procedure reviews can unnecessarily reduce access to care or the length of stay for children in residential settings.[59] It found that “even for residential mental health providers who are in-network with commercial health insurers, insurers’ utilization review and reimbursement practices can represent a significant barrier to access.”[60] Additionally, as noted above, QRTPs are required under federal law to conduct ongoing needs assessments to ensure that children meet clinical criteria for residential care.
It is often said that residential care should be “used only as a short-term, targeted intervention.”[61] This misconception helps drive policies like utilization review, which needlessly drives down lengths of stay at residential treatment facilities. As noted above, shorter stays can lead to negative consequences for these children. Longer stays, particularly for more acutely sick patients, provide stability that can result in better clinical outcomes. Sufficient time in residential treatment is associated with reduced readmission, better educational outcomes, long-term benefits, and improvement in problem behaviors—indeed, longer stays benefit “not only the youth and their families, but society by reducing the societal cost (e.g., lost wages, crime) when an at-risk youth does not receive sufficient treatment.”[62]
Conclusion: Learning from Deinstitutionalization and Recommendations for Reform
Reports of abuse, neglect, underfunding, overcrowding, and inhumane conditions at adult psychiatric hospitals during the mid-20th century gave rise to the deinstitutionalization movement aimed at closing them down. The movement gained popular appeal but was propelled by a small, passionate group of advocates who believed that “the rehabilitation of human warehouses, euphemistically labeled ‘state [psychiatric] hospitals,’ is a hopeless task” and “adding good psychiatrists to such institutions is like pouring good wine into a bad barrel…. There is only one way to deal with state [psychiatric] hospitals . . . empty them, close them, then blow them up.”[63] Over a few decades, the movement successfully eliminated hundreds of thousands of psychiatric beds.
In the mid-1970s, the National Institute of Mental Health (NIMH) released a groundbreaking report criticizing the deinstitutionalization movement.[64] The report identified the “largely unanticipated consequences . . . of a dysfunctional nature” created by deinstitutionalization and the growing concern for “the fate of a specific group of patients: those who would have been or would be likely candidates for long-term hospitalization but who, because of the decline of the state mental hospital, are now residing elsewhere.”[65]
We are still facing those consequences today.[66] As a 2008 report from the Assistant Secretary for Planning and Evaluation of HHS explained, the mental health system “suffers from significant capacity constraints for psychiatric inpatient services. Beginning in the 1960s, deinstitutionalization, defined as placing psychiatric patients in outpatient and community-based treatment facilities, has resulted in significant psychiatric bed shortages.”[67]
The dynamics that drove deinstitutionalization are driving the current decline in youth residential mental health treatment. Once again, widely reported but isolated instances of abuse and neglect have successfully been marshaled by a few passionate advocates seeking to close residential treatment programs. The results have been eerily similar to deinstitutionalization. Reduced access to residential treatment, like the reduction in adult psychiatric beds, is exacerbating pressures in criminal justice and other systems that serve troubled youths.
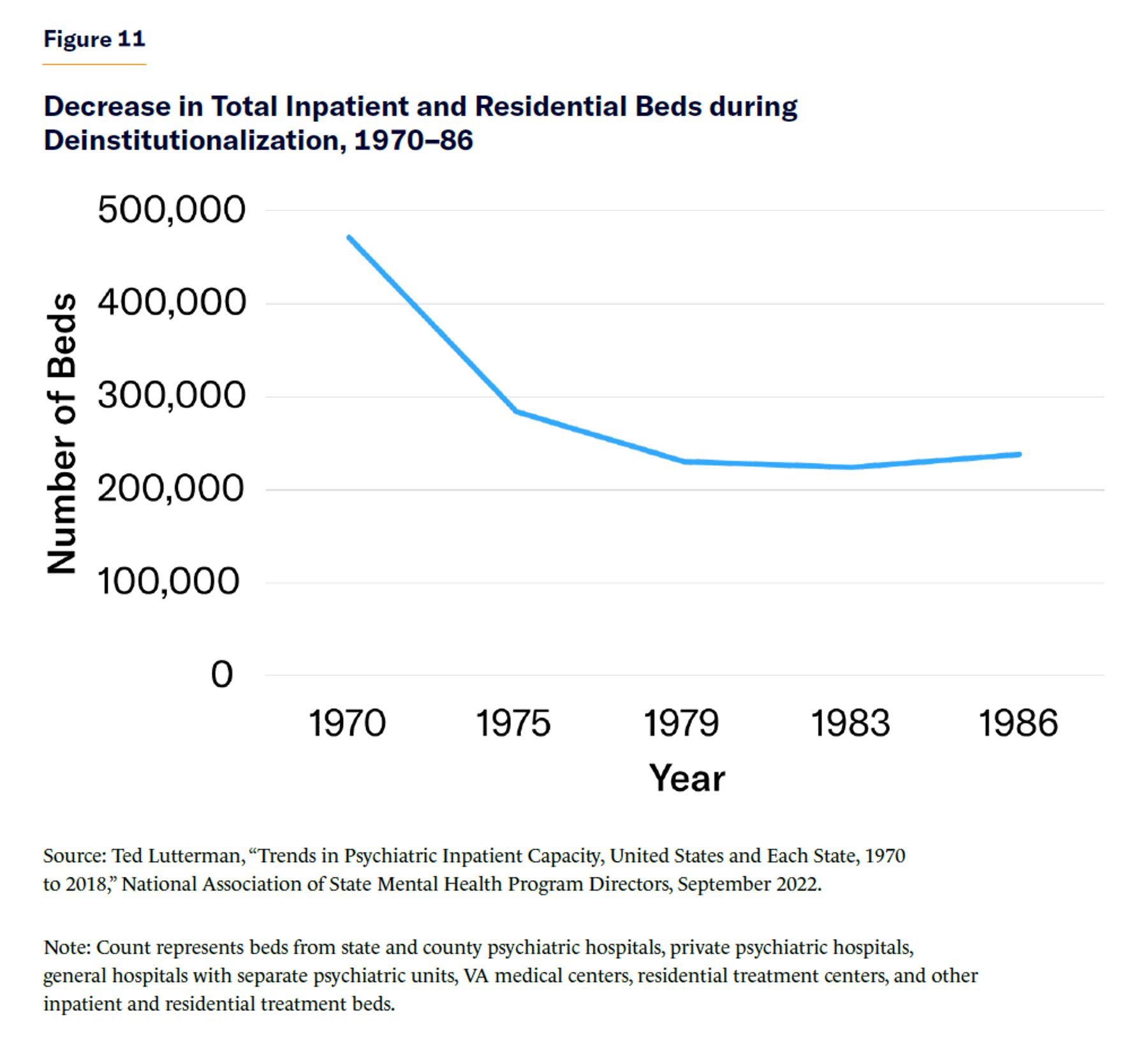
The number of beds in psychiatric hospitals declined during the core years of deinstitutionalization (1970–83) by about 52.3% (Figure 11). The number of beds in youth residential treatment facilities, by contrast, has declined by 66.2% (2010–22). In roughly the same period, the number of youth residential treatment beds declined 14 percentage points faster than adult psychiatric beds during the heart of deinstitutionalization. Deinstitutionalization triggered a cascade of adverse outcomes for the seriously mentally ill, including increased ED boarding,[68] incarceration,[69] and suicides.[70] By continuing to restrict access to residential youth mental health programs, policymakers risk repeating the mistakes of deinstitutionalization.
The clinical intensity, restrictiveness, and separation from family and community that are inherent in residential treatment have led some opponents to suggest that simply being placed in such a setting is an adverse outcome. This is based on a misconception about what constitutes effective care for youth with serious mental health challenges.
It is important for children to be cared for in the least restrictive, most family-like, setting possible. Occasionally, when children are very ill, that setting is residential. A functioning continuum of care provides access to the appropriate level of care based on clinical need and ensures access to that level of care for the appropriate duration of time. The right type of treatment and the right dosage are both needed. Denying or limiting care at any level, including residential, risks the prognosis for the child and is particularly harmful to vulnerable subpopulations, such as children in foster care. Despite evidence against shorter stays, policies—at both the state and federal level—encourage them. A blanket preference for shorter stays in all circumstances makes it harder for children to recover and makes it more difficult to operate residential programs. There are, and will remain, a subset of children with serious emotional disturbances for whom residential treatment is clinically appropriate and vital to their well-being.
Data and clinical evidence should inform policy to improve access to residential treatment. Some policy changes to achieve this:
- Addressing the IMD exclusion: For nearly 60 years, the Institution for Mental Diseases (IMD) exclusion has artificially limited access to inpatient and residential behavioral health care. Despite the exemption from the IMD exclusion for individuals under 21, the policy continues to limit youth access to residential treatment. States should be given more flexibility under the IMD exclusion to increase access to residential treatment programs.
- Enhancing §1115 State Medicaid Waivers: §1115 waivers allow states to innovate in their Medicaid program in ways that would otherwise not be permitted under Medicaid. Expanding their use will provide relief to states that have been limited by CMS’s strict, and sometimes unworkable, interpretation of PRTF and QRTP regulations and allow them to come up with new approaches to treating this patient population.
- Expanding the provider base: According to the American Academy of Child and Adolescent Psychiatry, there are “only 14 child and adolescent psychiatrists per 100,000 children in the country.” Increasing the number of child and adolescent psychiatrists and youth behavioral health-care providers will make it easier to expand services and reduce pressure on the few remaining residential treatment programs.
- Increasing access to other levels of care: Improving timely access to other levels of behavioral health care can reduce pressure on residential treatment programs. There is limited access to the levels above (inpatient) and below (partial hospitalization and intensive outpatient) residential treatment. Easing access to these levels will reduce the burden on residential providers.
- Allowing funds to follow the child: When children need to travel for access to residential treatment, it can be difficult to secure the resources that they would be entitled to if they stayed in their home community. Policies should ensure that funds, particularly education funding, follow the children to their place of treatment. This will address the long-standing issue of underpaying residential treatment programs for the education services that they provide, and it will allow students to return to school at the appropriate grade level after discharge.
These reforms would ease downward pressure on residential treatment, allow for an expansion of residential mental health treatment services, and improve patient care. These policies can help provide clinically appropriate and therapeutically supportive residential care. That will mean a greater chance that children with serious emotional disturbances will lead full lives in the community—instead of being relegated to the emergency department, onto unsheltered streets, or in jails and prisons.
About the Author
Scott Dziengelski is a consultant at King & Spalding, where he is a member of the Washington, D.C. office’s Life Sciences and Healthcare Industry group. Prior to joining King & Spalding, Scott was the director of policy and regulatory affairs at the National Association for Behavioral Healthcare (NABH). Scott also worked in the House of Representatives as a legislative director and for the House Energy and Commerce Committee. He is the recipient of the United States Capitol Police Medal of Merit and the American Academy of Child and Adolescent Psychiatry’s Friend of Children’s Mental Health Award.
Endnotes
Photo: Imgorthand/E+ via Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).