Slowing Optional Medicaid Spending Growth

Photo by baona/Getty Images
Introduction
Medicaid is the primary source of health care for low-income Americans. But the federal government distributes funding for the program according to how much states spend on beneficiaries—without any upper limit.
As a result, Medicaid expenses have risen uncontrollably. Over recent decades, it has been the fastest-growing federal program, with expenditures surging from $41 billion in 1985 to $824 billion in 2022. The richest states with the deepest tax bases have been able to claim the most in federal funding: in 2021, Alabama received only $7,052 in federal Medicaid funds per poor resident, while Delaware was able to claim $24,639.
Although the federal government requires states to provide a core package of health-care benefits to low-income parents, children, elderly, and disabled Americans, 63% of Medicaid spending goes to expanding eligibility and benefits beyond what is required—accounting for most of the differences between states.
Legislators have tried to cap Medicaid funding since the program’s early years. But the program’s costs often increase for complex reasons (such as growing caseloads of poor residents, new diseases or medical capabilities, and the aging of the population), which states may not be able to control. Congress has therefore struggled to design a reform of Medicaid financing that cuts the fat without scraping the bone.
Such a reform can be achieved by distinguishing the program’s mandatory acute-care spending from expansions of eligibility and benefits made at the discretion of states. The latter expenditures can more easily be controlled by states because they are less rigidly prescribed by the federal government and are less susceptible to unavoidable cost increase due to the business cycle. While full matching funding for mandatory services should be preserved, Congress should limit the annual increase in funding that states may claim for other Medicaid benefits, with the highest-spending states subject to tighter caps.
Medicaid’s Uncontrolled Spending Growth
Medicaid is two seemingly contradictory things: a health-care benefit for the poorest Americans; and a system of federal grants that goes disproportionately to the wealthiest states.
Medicaid is operated by states under federal rules, with a blend of state and federal funds. State Medicaid programs must cover a core package of medical benefits (hospital procedures, physician services, and nursing-home care) for anyone whom states make eligible for coverage, a group that must include low-income parents, children, elderly, and disabled Americans. States may also expand the package of covered benefits (to include dental care, prosthetics, rehabilitation, therapy, home health, and social services) and may expand eligibility to other low-income adults and higher-income families.[1]
Congress has repeatedly expanded the set of medical services that must be covered and the share of the low-income population who must be made eligible for Medicaid benefits.[2] But all states have eagerly expanded Medicaid programs beyond the bare minimum required by federal law.
For every $1 of their own that states spend on providing covered medical services to eligible beneficiaries, states may claim between $1 and $9 in “matching funds” from the federal government—without limit. Overall, two-thirds of the cost of Medicaid is borne directly by the federal government. This presents an extraordinarily lucrative arrangement, which every state has been eager to take advantage of. Although the poorest states do receive a higher federal matching rate for every dollar spent, the wealthier states with the deepest tax bases can put up many more dollars, and so are able to claim more federal funding. In 2021, for example, Delaware received $24,639 in federal Medicaid funding per poor resident, whereas Alabama received only $7,052.[3]
The great variation in expenditure by state reflects major disparities in eligibility. The number of Medicaid beneficiaries per poor resident ranges from 1.0 in Wyoming to 2.2 in Connecticut.[4] There are also enormous differences in breadth of long-term-care benefits covered by Medicaid programs, the use of asset tests in assessing eligibility for them, and the degree to which states seek to secure repayment from estates to cover the cost of services delivered.[5] Over recent years, states have increasingly used Medicaid waivers to claim federal funding for nonmedical services that yield incidental health benefits to their low-income residents.[6]
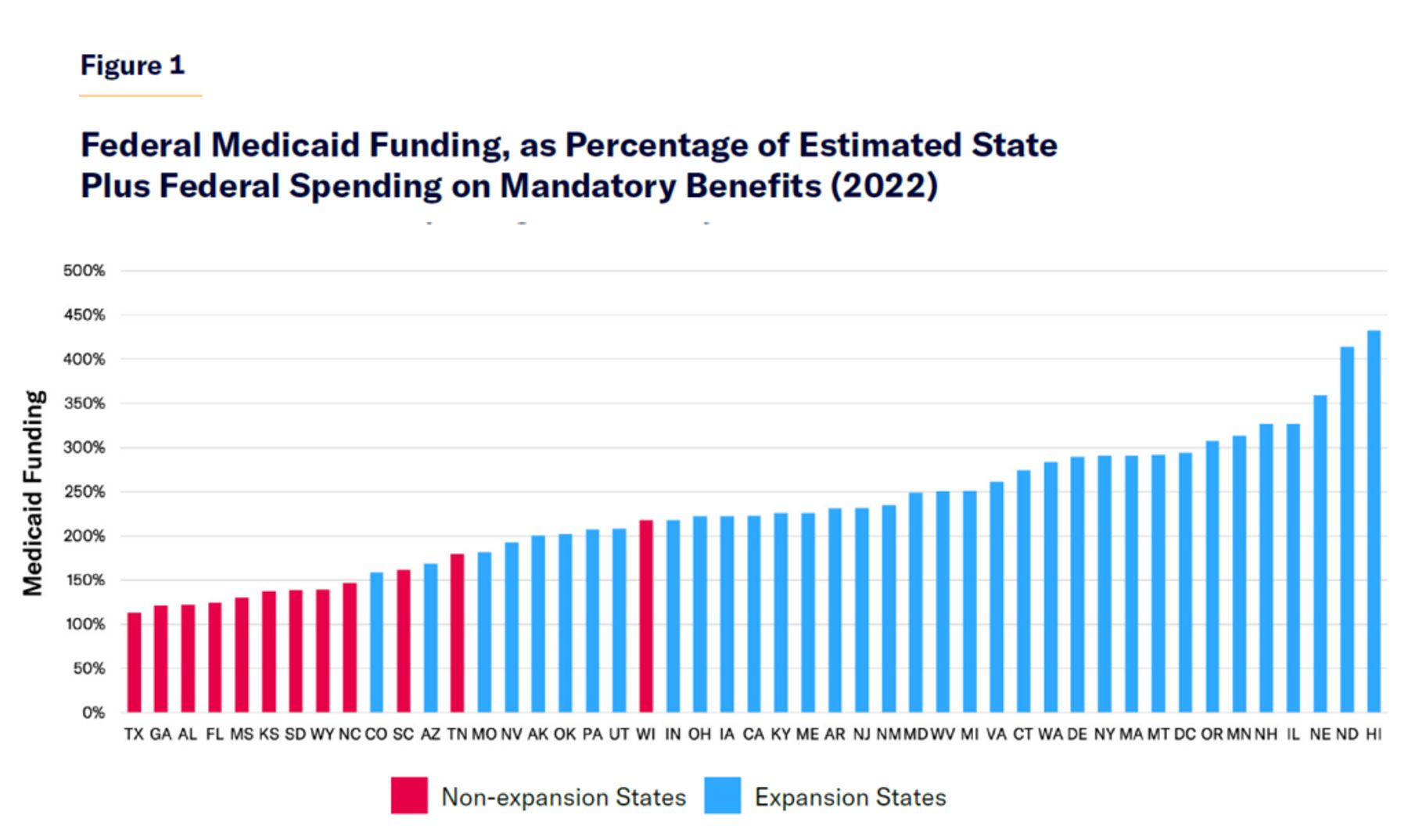
In 2022, in every single state, the total amount of Medicaid funding contributed by the federal government exceeded the combined federal-plus-state cost of mandatory Medicaid spending. Federal Medicaid funding ranged from 113% of the cost of mandatory benefits in Texas to 432% in Hawaii, averaging 208% nationwide (Figure 1). Optional expansions of benefits and eligibility account for 63% of Medicaid spending. Only a small part of the variation in federal funding for states—and 22% of Medicaid spending in 2022—is explained by decisions to expand eligibility under the Affordable Care Act (ACA).[7]
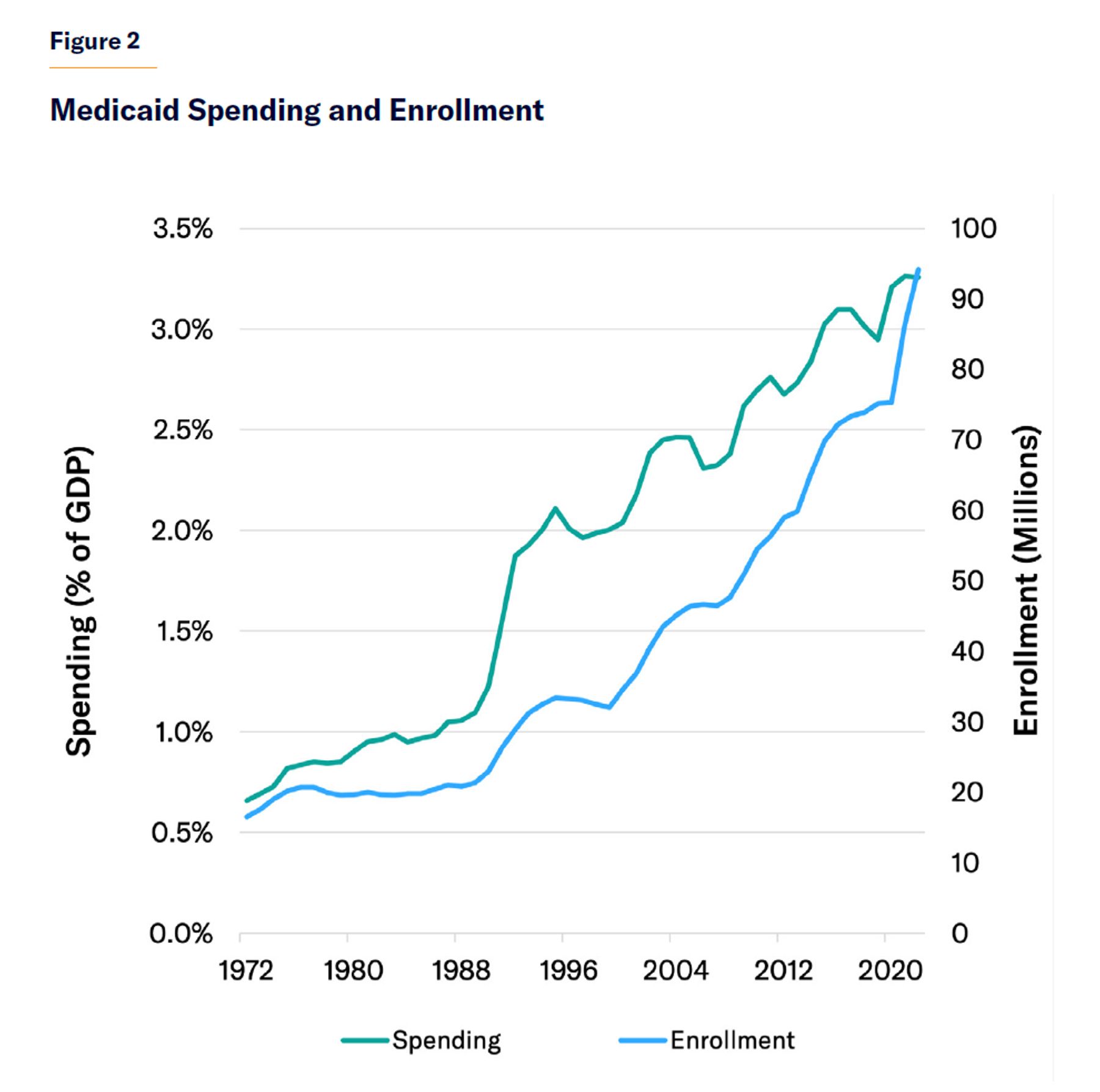
Medicaid spending has grown rapidly over the past four decades. From 1985 to 2022, combined federal and state Medicaid expenditures rose from $41 billion to $824 billion, in current dollars. This is partly due to rising health-care costs but owes much to the repeated expansion of the program’s eligibility. Over the same period, the program’s enrollment increased from 20 million to 94 million.[8]
States often expand Medicaid eligibility during times of macroeconomic prosperity, when their tax revenues are growing and the number of low-income residents enrolled in the program declines. In recessions, when revenues slump and program costs surge, they have typically been able to secure federal bailouts. The upshot is a ratchet effect, whereby every business cycle leads to a higher level of enrollment and expenditure (Figures 2 and 3).[9]
As Medicaid eligibility has repeatedly been expanded, additional expenditures have done less to extend benefits to the uninsured. It has been estimated that 60% of some coverage expansions served only to displace private insurance coverage.[10]
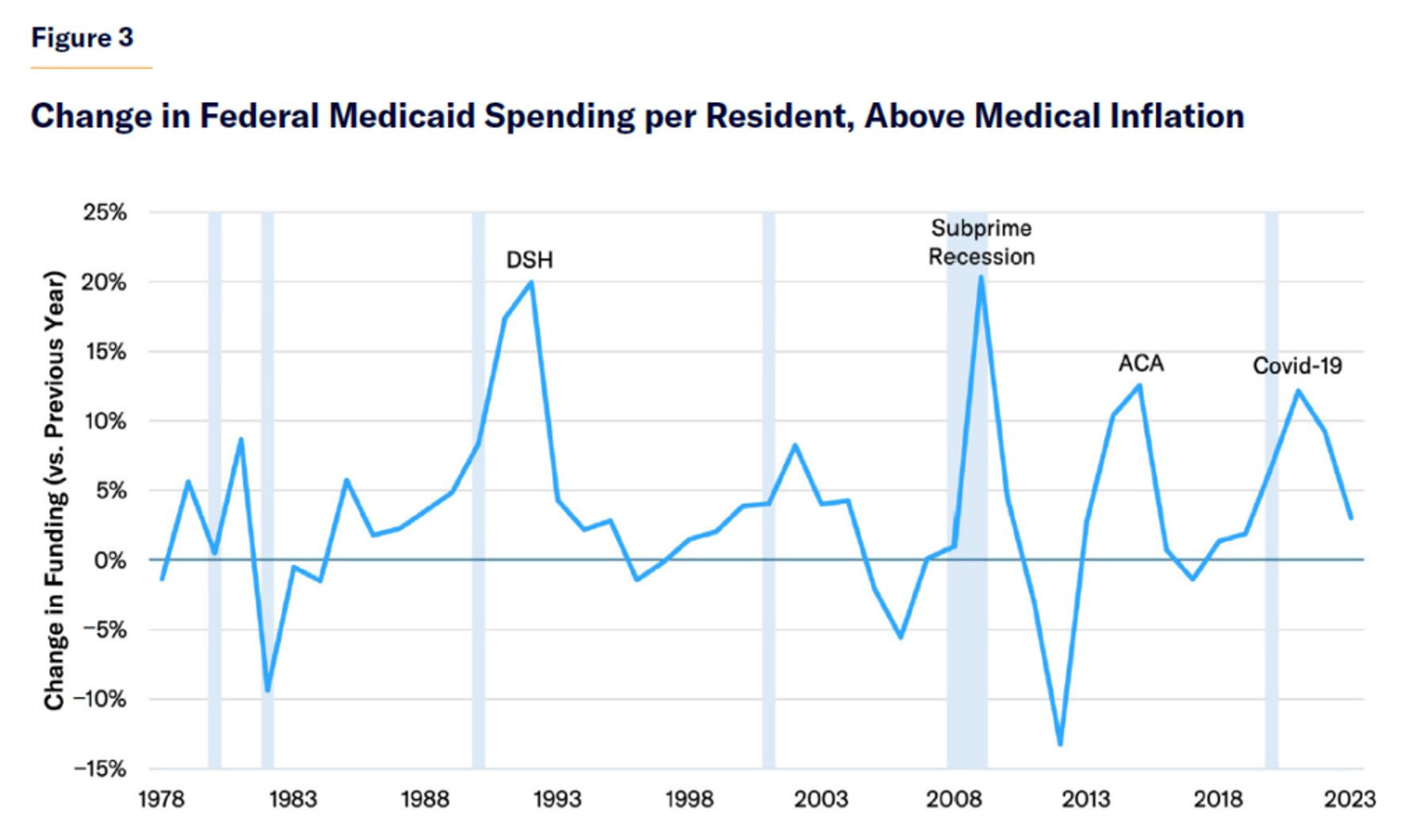
DSH: Disproportionate Share Hospital (DSH) Payments
Source: OMB, historical tables, “Table 8.5—Outlays for Mandatory and Related Programs: 1962–2029”; U.S. Bureau of Labor Statistics, Consumer Price Index for All Urban Consumers: Medical Care in U.S. City Average (CPIMEDSL), retrieved from FRED, Federal Reserve Bank of St. Louis; National Bureau of Economic Research (NBER), Public Use Data Archive, “U.S. Business Cycle Expansions and Contractions,” updated Mar. 14, 2023; World Bank, Population, Total for the United States, retrieved from FRED, Federal Reserve Bank of St. Louis.
The separation of Medicaid’s administration (by states) and its financing (predominantly by the federal government) has encouraged states to inflate the program’s cost.[11] This has not only led states to expand benefits and enrollment; it has also allowed a greater degree of fraud, waste, and abuse than they would have tolerated if states were required to fully pay for Medicaid expenditures. Improper payments may account for up to 25% of the cost of Medicaid.[12]
It has also led states to weakly enforce asset tests associated with eligibility for long-term care—thus forcing the federal government to fund nursing-home and home health services for millions of Americans who could have purchased private long-term-care insurance for themselves.[13] Nor do states appropriately recover costs from estates that have profited from Medicaid payment for services. Various states now claim Medicaid funds to pay residents to “sit at home” with their elderly relatives—with the cost in New York alone surging from $0.3 billion in 2016 to $9.1 billion in 2023.[14]
Notoriously, all 50 states have increased the fees that their Medicaid programs pay for hospital services, thus entitling them to higher reimbursements from the federal government, while simultaneously imposing taxes on those facilities to finance the supposed state contribution to the program’s expenditure.[15] Often, states have used publicly owned hospitals to capture Medicaid funds as a way to improve their general fiscal situation.[16]
States have increasingly received waivers from Medicaid’s standard rules, allowing them to inflate federal payments for medical services, claim funds for residents who are ineligible for the program, and gain Medicaid funds for non-health-care services.[17] States have similarly sought to evade accountability for federal funds by deliberately underpaying medical providers serving covered beneficiaries, so that they can employ funds for unapproved purposes.[18]
Although Congress and various federal agencies have spent decades trying to rein in Medicaid costs, improper payments, and kickback schemes involving states, insurers, and medical providers, they have done little more than divert the flow of funds.[19] So long as federal matching funds for state expenditures are uncapped, states will find creative ways to circumvent restrictions on matchable spending, and federal authorities will find themselves playing Whac-A-Mole with futile attempts to prevent unintended expenditures.[20]
Attempts to Cap Federal Medicaid Funding
Legislation to cap Medicaid matching funds has repeatedly been advanced, but never enacted.
Every matching-fund program established by the Social Security Act of 1935 (including Old Age Assistance, Aid to the Blind, and Aid to Dependent Children) included a cap on aid to states. These caps were maintained when the Social Security Act Amendments of 1950 allowed states to claim federal matching funds for “vendor payments” to finance the provision of health-care services to beneficiaries of these programs.
In 1960, the Kerr-Mills Act established an additional system of federal matching aid for states to fund health-care services for the elderly poor, but it did not cap the amount of aid that states could claim. Political scientist Shanna Rose notes: “Although it went largely unnoticed at the time, the adoption of open-ended matching grants was unprecedented; federal funding for public assistance programs had always been capped.”[21] Kerr-Mills was the prototype for Medicaid, which was enacted, along with Medicare, in 1965.
Within two years of the program’s enactment, New York had expanded eligibility for its Medicaid program to such an extent that its spending alone exceeded what had been expected for the entire country. To rein in costs, Medicaid’s legislative architect, House Ways and Means Committee Chairman Wilbur Mills (D-AR), proposed capping annual federal funding for each state under the program at $12 per capita. But the proposal was blocked after political pushback from governors, and, in 1967, Congress instead opted to cut costs by narrowing eligibility.[22]
By 1976, the cost of Medicaid had continued to grow, so President Gerald Ford proposed consolidating Medicaid and other health aid programs into block grants, with federal funding uncoupled from state contributions.[23] Ford’s FY 1978 budget also proposed gradually shifting the distribution of federal Medicaid funding to align with the poor population of each state, its per capita income level, and its “tax effort.”[24] Neither reform was enacted.
From 1975 to 1981, Medicaid spending grew at an average of 16% per year.[25] In his first budget, President Ronald Reagan proposed capping the increase of federal Medicaid spending at 9% starting in 1982, and then increasing it with inflation in subsequent years. This proposal passed the Senate but was dropped in conference committee, due to opposition from a coalition of House Democrats and Northeastern Republicans.[26]
The 1981 Omnibus Budget Reconciliation Act nonetheless consolidated various other social-services grant programs into block grants. Reagan’s budget proposals in 1986, 1987, and 1988 proposed to similarly distribute Medicaid funding as block grants, with federal funding to increase at the same rate as the medical consumer price index (CPI-M).[27] Again, none of these proposals was implemented.
In 1994, after Republicans secured majorities in both houses of Congress, they sought to distribute funding for all joint state-federal means-tested welfare programs as block grants to states—while removing the legal entitlement of individuals to federally defined benefits.[28] The legislation would have distributed “MediGrant” funds between states according to their number of poor residents, their relative medical needs, hospital wages, and past Medicaid spending levels.
MediGrant was designed to narrow disparities in aid to states over time, and it would have reduced federal Medicaid spending by 15% nationwide in 2002 (ranging from a 45% cut in Alaska, but exceeding eventual payments to Texas and West Virginia). The sweeping welfare reform package passed the House and Senate; President Bill Clinton initially vetoed the bill, signing it into law only after successfully demanding that its changes to Medicaid be dropped.[29]
Clinton wanted to maintain individuals’ entitlement to Medicaid coverage and for payments to states to increase in line with enrollment.[30] As an alternative to block grants, his FY 1997 and 1998 budget requests proposed capping the level of federal Medicaid spending per enrollee. At the time, the Clinton administration claimed that this reform would have reduced Medicaid spending by 7%. But administration officials later argued that the proposed caps were merely an attempt to deflect the political force of Republican proposals and were not designed to yield significant savings.[31]
In 1997, with the Republican Congress opposed to expanding an uncapped Medicaid program, the budget agreement with the Clinton administration established the Children’s Health Insurance Program, whereby the federal government would provide $2–$5 for every $1 that states spent on eligible beneficiaries, up to a cap. This program did not establish any specific entitlement to care for individuals, but its expenditures were set to increase automatically every year, without appropriations, according to the rate of increase in national per capita health-care spending and the child population in each state.[32] From 2003 to 2023, CHIP spending increased by more (416%) than Medicaid (383%).[33]
In its FY 2012 budget resolution, the House Budget Committee proposed converting federal Medicaid funding for states into block grants, a proposal that was endorsed by the 2012 and 2016 Republican Party platforms.[34] In 2013, Representative Fred Upton (R-MI) and Senator Orrin Hatch (R-UT) embraced caps on the rate of growth of federal spending per Medicaid enrollee, similar to what President Clinton had previously endorsed.[35] In 2016, House Speaker Paul Ryan (R-WI) proposed allowing states to choose between receiving Medicaid funding through either per capita caps or block grants.[36]
After the election of President Trump gave Republicans a chance to reform the ACA, the House in May 2017 passed the American Health Care Act (AHCA). AHCA capped the annual increase of Medicaid matching funds per enrollee for children and able-bodied adults at the rate of medical inflation (CPI-M), and for disabled and elderly beneficiaries at 1 percentage point above CPI-M. These caps would not apply to federal matching funds for subsidies to “Disproportionate Share Hospitals” or to Medicare cost-sharing. States could alternatively opt to receive the capped amount of Medicaid funding as a 10-year block grant.[37]
In June 2017, during the GOP’s attempt to replace the ACA, the Senate considered the Better Care Reconciliation Act (BCRA), which contained similar provisions but would have increased caps according to the lower rate of general inflation (CPI) beginning in 2025. The bill further proposed allowing CMS to adjust each state’s annual caps by 0.5%–2%, depending on their relative levels of spending per enrollee.[38]
The GOP’s failure to replace the ACA in 2017 was widely attributed to proposed cuts to Medicaid that would have been enacted. But 99.6% of these cuts would have come from a reduced matching rate for able-bodied adult enrollees, rather than being reduced by per capita caps.[39] Because the caps proposed by AHCA were set above the likely increase in per-enrollee spending, and could easily have been circumvented by inflating the number of enrollees with slow-growing costs in each category, they would have done little to slow the overall growth of Medicaid spending.[40]
The Reform Challenge
Caps on Medicaid funding for states have been hard to enact, even under unified Republican control of government, due to the difficulty of pre-specifying reasonable levels of assistance.
Voters tend to punish politicians who cut existing public entitlement programs, despite often being supportive of those who resist expanding these programs.[41] One of the most politically effective methods of reducing expenditures over the long term is therefore to slow their rate of growth. This is particularly true for health-care programs, due to the “stickiness” of overhead costs associated with hospital care in particular. Although existing commitments to hospital facilities are hard to cut, decisions to expand facilities are highly influenced by expected future revenues.
To slow the growth of Medicaid expenditures that result from decisions made by states, it is necessary to determine a counterfactual level of spending that otherwise would have prevailed. This can be difficult because Medicaid costs may increase due to factors beyond the control of state policymakers, such as rising medical wages, the availability of newly developed treatments, and increasing volumes of procedures.
Medicaid is not just a method of distributing funds to states; it creates an entitlement to care for individuals. To receive federal funds, states must provide a predefined set of covered health-care services to all those eligible, with payments to medical providers sufficient to assure access to care—and they must do so without requiring premiums or more than nominal out-of-pocket expenses, and without imposing other barriers to essential services. Governors of both parties are highly sensitive to the risk of being required by federal law to increase spending on benefits without receiving additional funds for the purpose.
Over the longer term, the cost of Medicaid is pushed up by an aging population, which has more complex edical needs and requires more long-term-care assistance. Although proposed caps have attempted to make specific allowances for such unavoidable increases in medical costs, they have done so imprecisely, and thus threatened arbitrary cuts without greatly constraining the avoidable increase of expenditures.
In the short run, states are also often forced to increase their Medicaid expenditures as caseloads increase for reasons out of their control—such as recessions, epidemics, or natural disasters. Although current matching-fund arrangements only partly absorb increases in program costs, a crude cap on total federal Medicaid funding for each state would leave states responsible for the entirety of exogenous increases in program costs. Most governors view this as intolerable, as states are unable to run short-term budget deficits, and would therefore be forced to increase taxes or cut benefits when the pain of doing so is greatest.
For this reason, Democrats and, later, Republicans have tended to prefer “per capita caps”—that is, limits on federal funding per enrollee. Such caps would not increase the exposure of states to business-cycle risks. But nor would they do much to constrain increases of expenditure, which have mostly resulted from expansions of eligibility for benefits. In fact, states could get around caps on the growth of federal per-enrollee spending simply by expanding eligibility to relatively healthier enrollees.
While loose per-enrollee caps on the growth of funds for states would do little to constrain the expansion of Medicaid’s cost to federal taxpayers, excessively tight caps would increase the prospect of ad hoc bailouts—making the arrangement similarly pointless. This is already a problem, as impromptu expansions of federal funds were provided to assist states in dealing with recessions in 2001, 2003, 2009, and 2020.[42]
Any attempt to cut Medicaid costs by slowing the growth of spending is further complicated by great differences in existing levels of funding distributed to states. A uniform cap on the rate of increase of federal funding for each state would most constrain the states that currently receive the least—those that already offer the most meager benefits, keep costs best controlled, and typically have the shallowest tax bases of their own.
Switching to block grants would likely do little to constrain the growth of Medicaid spending. The federal government would need to constantly monitor states to prevent diversion of funds to extraneous purposes, as has been the case with Temporary Assistance for Needy Families (TANF) or Medicaid waivers.[43] The distribution of funds through block grants would also likely increase pressure for ad hoc federal bailouts according to the business cycle.[44] Block grants created as options for states that switch from the current model would be chosen only by states that saw them as a way to increase federal funding—for instance, those with declining populations.
Reform Proposal
The rate of increase of federal funding for noncore Medicaid benefits should be limited according to each state’s levels of overspending, as defined by the extent of their expenditure on optional services. Annual federal funding for Medicaid, distributed to states according to the Federal Medical Assistance Percentage (FMAP), should be subject to these additional limits:
- Core (mandatory acute-care and drug benefits for mandatory enrollees):
– Capped according to risk-adjusted estimate of Medicaid mandatory acute-care and prescription drug costs at Upper Payment Limit rates.[45] - Auxiliary (all other benefits):[46]
– Growth per resident capped at CPI-M for states with total federal funding >250% cost of all mandatory spending
– Growth per resident capped at CPI-M + 1 for states with total federal funding 175%–250% all mandatory spending
– Growth per resident capped at CPI-M + 2 for states with total federal funding 100%–175% all mandatory spending Slowing Optional Medicaid Spending Growth
Full matching funding shall be permitted for the cost of providing mandatory benefits to mandatory enrollees. The growth of matching funds for other spending would be capped—with the cap being tighter for states where total spending is higher relative to mandatory spending.
Eligibility and risk adjustment determinations should be federalized for mandatorily eligible enrollees, to prevent states from inappropriately reclassifying enrollees to avoid the cap on federal matching funding for other benefits. Additional flexibility should also be provided for states to cut optional benefits for mandatory enrollees and benefits for optional enrollees.
Justification
Capping the growth of optional Medicaid spending would preserve essential funding while inhibiting the expansion of extraneous expenditures.
The growth of Medicaid spending is due less to “waste” or “inefficiency” than to expansions of benefits and eligibility. Capping the growth of optional Medicaid spending would make states responsible for paying for increases in the program’s expenditures that they choose to incur. This would remove the subsidy for states to expand Medicaid at the expense of other spending priorities or cutting taxes.
The permitted level of matching funding for core benefits would increase automatically with the cost of covering mandatorily eligible beneficiaries—whether due to increased enrollment during recessions or to rising medical costs as beneficiaries age. This would not exacerbate funding shortfalls in macroeconomic downturns, but it would inhibit the use of any temporary increase in federal funding to permanently expand eligibility and the scope of benefits.
The “auxiliary benefit” category would group together optional acute-care expenditures and long-term-care benefits. Unlike eligibility for Medicaid among workers in the labor force, Medicaid spending on long-term-care benefits and medical care for the elderly or disabled does not fluctuate greatly with the business cycle. Caps for spending on auxiliary benefits therefore do not need to be adjusted for short-term shifts in circumstances, unlike those for core benefits. When states expand eligibility for Medicaid acute-care benefits beyond mandatory groups, such as to able-bodied adults under ACA, the federal government already assumes 90% of the cost and hence most of the fiscal risk. To the extent that any states choose to expand eligibility and incur business-cycle risk beyond this level, they should be expected to pay for it themselves.
Caps on the growth of funding for auxiliary benefits would not threaten the entitlement to core benefits—rather, they would encourage states to focus resources on these benefits. Allowing federal funding per resident for auxiliary benefits to increase at the rate of medical inflation (CPI-M) would enable all states to maintain the existing level of optional benefits for existing enrollees. But only currently low-spending states would be able to claim increases in federal funding beyond this level. The greatest impact of the cap would therefore be to slow unilateral expansions of benefits and eligibility by the most highly subsidized and wealthiest states.
As with spending on optional benefits, current levels of spending on long-term-care services vary enormously from state to state, as the nature of services provided is not bound by a precise uniform definition. Rules requiring states to provide home health services to individuals requiring a “nursing-home level of care” and those specifying needs in terms of “activities of daily living” are too vague to meaningfully shape the level of expenditure that states determine to be desirable.
It is therefore not possible to determine an objectively “correct” quantity of funding for long-term care and optional benefits. But the appropriateness of funding levels can be assessed relative to the status quo, by comparison with other states, and as a factor of spending on mandatory benefits. The cost of core benefits is a good benchmark against which to judge excessive Medicaid spending levels, as it reflects the size of the Medicaid population, the extent of its medical needs, and the cost of delivering care in a particular geographic area. It is also a metric that can be determined independently by the federal government.
At current levels of Medicaid spending, roughly one-third of states would see caps on federal funding for auxiliary benefits per resident increase every year by the rate of medical inflation (CPI-M); another third of states would see caps increase by 1 percentage point more than CPI-M; and the final third would see caps increase by 2 percentage points more than CPI-M.
To get a sense of the likely fiscal impact: in 2033, federal Medicaid spending would be no lower than the $879 billion level projected by the Congressional Budget Office (CBO) if auxiliary expenditures grew nationwide at 2 percentage points above CPI-M; it would be 3.6% lower ($848 billion) if auxiliary Medicaid spending increased at 1 point above CPI-M; and 8.5% lower ($804 billion) if auxiliary expenditures increased at CPI-M.[47]
Capping the total level of Medicaid funding that states can claim would limit their ability to inflate federal payments with provider taxes, claims for uncovered services, inadequate utilization management, gaming of FMAP disparities, managed-care state-directed payments, and bloated waiver benchmarks. It would also absolve the federal government of having to make often futile attempts to police such improper reimbursement requests.
Directly allowing for increased expenditures on mandatory acute-care benefits, which rise with the business cycle, would make it unnecessary to exempt from the caps spending increases due to rising enrollment. Unlike per-enrollee caps on the growth of matching funds for auxiliary benefits, per-resident caps could not be easily manipulated by state governments—by adding enrollees using minimal services—in order to inflate federal funding. Nor would per-resident caps require the establishment of multiple subcategory caps (such as for the disabled, elderly, parents, or children), which arise from the need to mitigate that manipulation.
In 2017, the bulk of Republicans’ proposed cuts to Medicaid came through reductions of FMAP matching funds for ACA’s expansion of the program to able-bodied adults. These cuts threatened severe, disruptive, and immediate reductions in revenue for most states, including many Republican states that received relatively little in federal funding. The unpopularity of FMAP cuts prevented the enactment of substantial and effective caps on the growth of the program’s expenditures.
Unlike cuts to matching rates, which threaten to take away existing benefits, caps can be designed to focus spending reductions on the highest-spending states with the most bloated optional benefits. That makes them easier to enact politically. But this reform is also a more complete solution to the problem of unduly inflated Medicaid expenditures, which exists mostly beyond the category of enrollees made eligible by ACA.
Conclusion
Currently, states are largely responsible for expanding Medicaid expenditures, while the federal government is largely responsible for paying for them. Caps would eliminate that misalignment, making states responsible for paying for any optional expansions to benefits or eligibility that they choose to make.
In the long run, this can be expected to increase scrutiny and debate about appropriate Medicaid expenditures. Congress would have more of a say over the purposes for which funds are allocated across states—rather than letting them be distributed without limit, according to the capacity of states to put in their own resources. There would be more focus, investigation, and debate about which benefits ought to be made mandatory—thus forcing greater consideration of trade-offs.
The design of caps could be finessed or tightened over time, once the principle is established. Congress may wish to further reduce the permitted growth of funding for auxiliary benefits, or it may wish to increase the share of mandatory benefits paid by the federal government. Indeed, caps may make it easier for states to be trusted with a greater rate of federal assistance where it is genuinely merited (for instance, to make up for lack of fiscal capacity, especially in recessions). This could reduce the risk and cost to states, without increasing expenditure on services beyond those intended.
By reducing the disparity in benefits between states over time, caps could also facilitate the gradual federalization of the program’s essential benefits—leaving states to pay for whatever additional benefits they choose to provide out of their own funds.[48]
Endnotes
Please see the Endnotes in PDF.
Photo by baona/Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).