Restraining Medicaid’s Budget-Busting Waivers

Photo: LPETTET/iStock/Getty Images Plus
Executive Summary
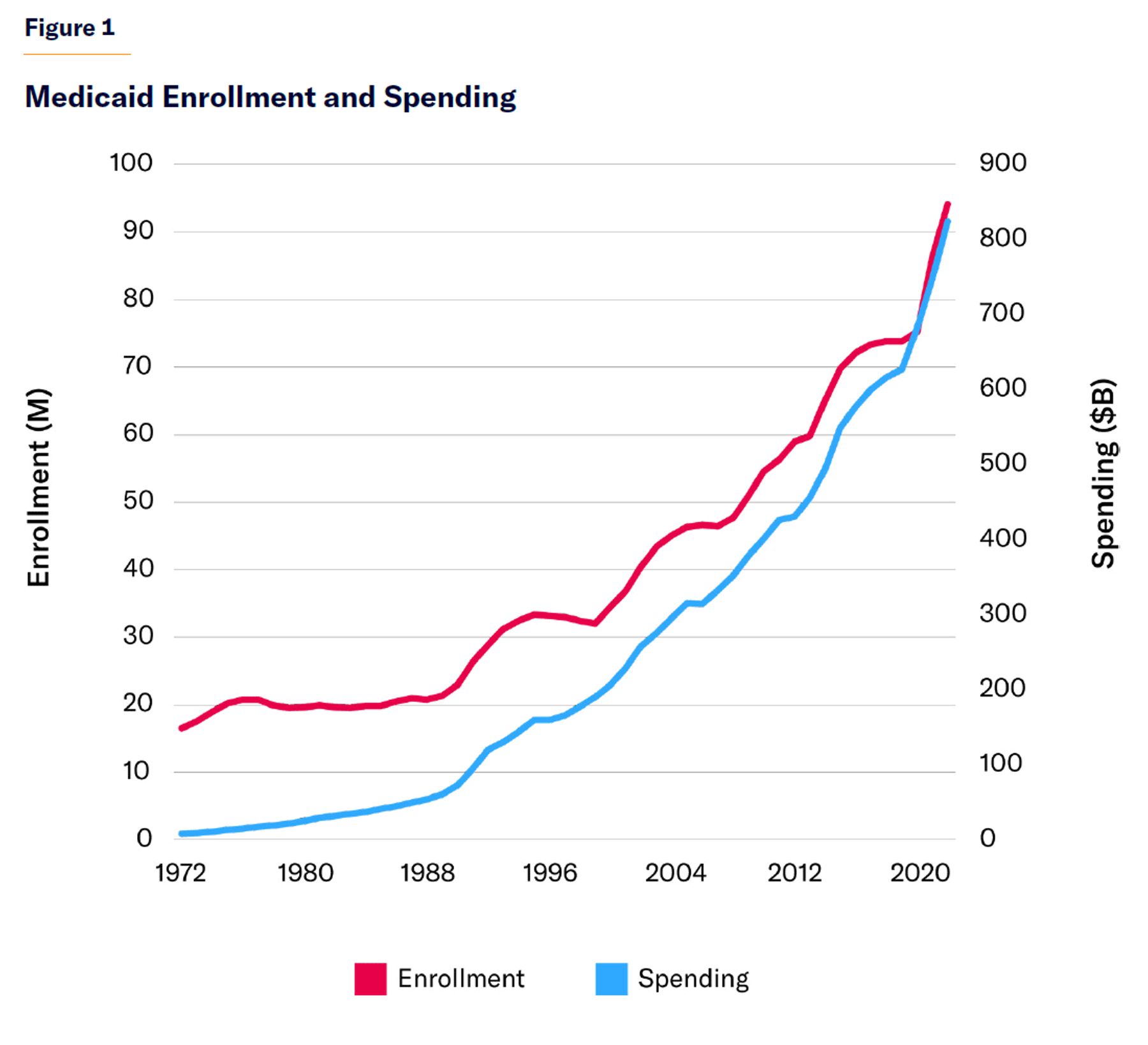
For decades, federal officials have tried to let states make Medicaid more cost-effective by waiving some of the program’s standard terms and conditions. But waivers have not led to savings for taxpayers. Instead, Medicaid spending has surged, from $205 billion in 2000 to $683 billion in 2019—with 75% of that spending now under a waiver.
Waivers provide no incentive for states to reduce the program’s overall expenditures, because waiver funding is contingent on states spending any purported savings that are generated. Not surprisingly, then, waivers have served as a one-way ratchet for increased Medicaid costs.
Increasingly, waivers have allowed states to claim federal matching funds for purposes that would not normally qualify, including housing, infrastructure, and even food benefits.
Most waivers are supposed to be budget-neutral, but that requirement has not proved to be an effective check on their use, because it is very difficult to objectively identify how much would have been spent without the waiver. Therefore, states can—and routinely do—inflate baseline costs in order to reap massive windfalls in federal matching funds.
Since waivers now account for the bulk of Medicaid spending, any fundamental reform of the program has to contend with their widespread abuse. This should be done by establishing a single unified spending cap—for both waiver and nonwaiver spending—for each state claiming waiver funds. This would allow federal officials to accurately set and enforce limits based on objectively comparable costs, while freeing states from the administrative burden and rigidity involved in futile attempts to police and evaluate idiosyncratic or overlapping waivers.
Introduction
Medicaid Waiver Background
Medicaid is a joint state-federal health-care system that delivers services to eligible low-income Americans. It is operated by states under broad federal rules. The federal government provides between $1 and $9 for every $1 that states spend on services covered by the program.[1] There is currently no upper limit on the amount of federal funding that states may claim under this arrangement.
The program’s size and cost have grown rapidly over recent decades (Figure 1). In 2022, Medicaid spent $824 billion on 94 million beneficiaries, with 71% of the cost borne directly by the federal government.[2]
States claiming federal Medicaid funds must cover a core set of hospital, physician, and long-term-care benefits for children, parents, disabled, and elderly Americans with the lowest incomes. They may also provide a more extensive set of benefits (including dental services, rehabilitation, or therapy services) to these groups and to a more broadly defined set of low-income Americans (including able-bodied childless adults).[3] Under this standard arrangement, federal funding expands and contracts in direct proportion to state spending on covered benefits.
Alternatively, states may opt to receive federal funds under a waiver from the program’s standard terms. The intent of this provision is to allow states to purchase medical services in innovative ways, and thus to improve the health of low-income residents with a given amount of federal aid.[4] States can use funds from Medicaid waivers for expenditures that would not normally be covered by the program.
For instance, former governor Andrew Cuomo suggested that a waiver would allow New York to achieve “a fundamental restructuring of its Medicaid program that achieves measurable improvements in health outcomes, sustainable cost control and a more efficient administrative structure.”[5] His reform proposal promised to save money by reducing avoidable hospital use by 25%.[6]
Medicaid waivers appeal Justice Louis Brandeis’s conception of states as “laboratories of democracy,” able to experiment with policy changes in a localized manner. Medicaid, a large, unwieldy, and diverse program, is difficult for Congress to manage effectively through legislation. Waivers help state officials alter the program’s benefit design, eligibility, and payment structures in response to local circumstances and opportunities without the need for congressional action.
States may claim federal Medicaid funds under two main kinds of waivers, named after the sections of the Social Security Act under which the statutory provisions are located.
§1115 “Demonstration” Waivers
These waivers were enacted in 1962 to allow then-secretary of Health, Education, and Welfare to waive specified sections of the Social Security Act, in order to permit “any experimental, pilot, or demonstration project which, in the judgment of the Secretary, is likely to assist in promoting the objectives” of the legislation.[7] When Medicaid (which was codified as Title XIX of the Social Security Act) was established in 1965, this authority was expanded to allow the secretary to waive provisions of Section 1902 of the legislation (which defines Medicaid’s standard benefit rules) for demonstration purposes.
§1115 waivers were originally intended to permit experiments in social-services delivery for periods of up to five years, such as funding training for caseworkers. Early Medicaid waivers were narrow and typically intended for local payment reforms. But increasingly, federal and state officials realized that §1115 waivers could be employed as a method of enacting sweeping changes to the structure of benefits through intergovernmental bargaining, thus circumventing the need for approval by Congress.
In 1982, Arizona’s entire Medicaid program was established through a §1115 waiver, under which the state would purchase services through managed-care organizations. Over the subsequent decade, §1115 waivers became an instrument to reform the Aid to Families with Dependent Children (AFDC) program; they were used to establish benefit time limits, work requirements, family caps, and other new terms of eligibility.[8] By the time that welfare reform legislation was passed in 1996, 75% of AFDC recipients were receiving benefits through systems operating under waivers.[9]
§1115 waivers can also be used to authorize nonstandard Medicaid expenditures, as long as they do not increase the federal budget deficit.[10] This is not a formal statutory requirement, but the Department of Health and Human Services (HHS) has required states to demonstrate “budget neutrality” for any spending under a waiver—i.e., to demonstrate that projected growth in enrollment and spending per beneficiary under the waiver would not exceed a base level associated with the existing program.[11] States may claim matching funds for waiver spending up to a limit, set as an aggregate total amount or with an adjustment for the number of individuals who receive benefits.[12] Program spending on nonmedical waiver benefits may not exceed 3% of total Medicaid expenditures, while states must exceed specified thresholds in paying providers of core medical services and maintain other levels of spending on social services.[13]
§1915 “Programmatic” Waivers
These waivers, established by the Omnibus Budget Reconciliation Act of 1981, allow two major types of changes to the Medicaid program.[14]
§1915(b) waivers sought to expand the use of managed care in Medicaid, by allowing states to restrict beneficiaries’ choice of medical providers. States can use such waivers to require all beneficiaries to enroll in managed-care organizations, and states can use the associated “savings” to provide additional benefits to low-income residents. These waivers are approved for renewable two-year periods.[15] To gain approval for §1915(b) waivers, states need only show that the spending would be cost-effective and efficient, rather than fully budget-neutral.
§1915(c) waivers are intended to allow states to provide home- and community-based long-term-care services to Medicaid beneficiaries who otherwise would require nursing-home care. They are typically used to help those with intellectual and developmental disabilities live more independently in the community—e.g., by providing deposits for housing costs or compensating relatives for looking after beneficiaries. States can use waiver funds to provide home-based services to residents who typically would not be eligible because of income and asset limits. But they may also target benefits by capping enrollment, establishing waiting lists, or limiting eligibility for particular services to certain geographic areas or to certain subsets of beneficiaries. States must demonstrate only that §1915(c) spending per enrollee is not higher than otherwise would be incurred in an institutional care setting.[16]
Waivers have proved particularly important in shifting Medicaid to managed care (which was utilized by 72% of beneficiaries in 2020) and in shifting long-term care into home- and community-based settings (which accounted for 59% of long-term-care expenses in 2019, compared with only 18% in 1995).[17] In recent years, §1115 waivers have increasingly been used to allow for population-based payments to providers.[18]
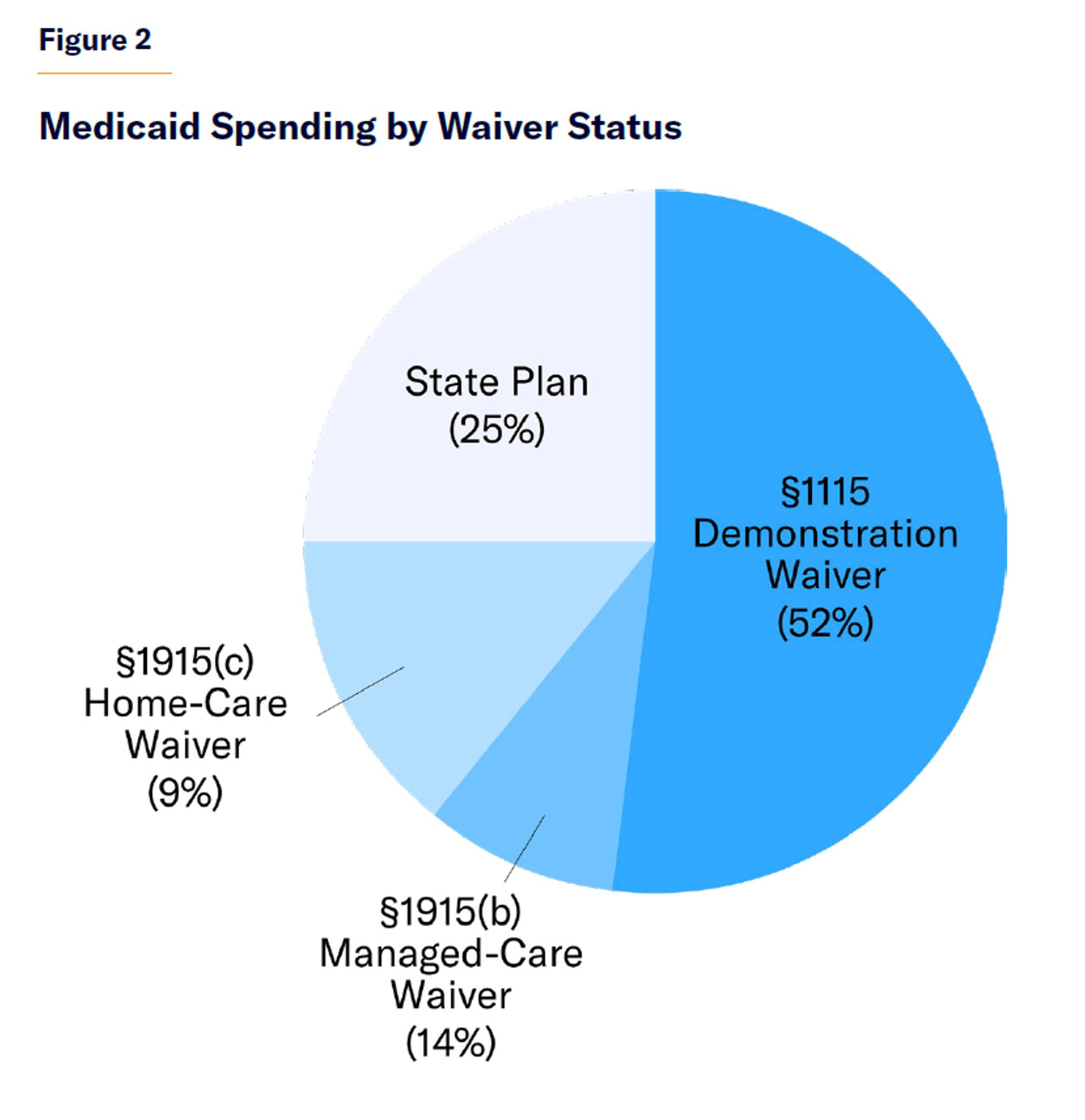
In 2019, 75% of all Medicaid spending occurred under a waiver: 52% through §1115 demonstration authority; 14% under §1915(b); and 9% under §1915(c) (Figure 2). Some $18 billion in spending under §1115 waivers went to things that would not otherwise have been entitled to federal matching funds, primarily “supplemental payments” to medical providers. In September 2021, there were 76 §1115 demonstrations in 47 states and the District of Columbia. The share of Medicaid spending under §1115 waiver authority exceeded 90% of total program spending in Arizona, Hawaii, Kansas, New York, and Vermont; but it was less than 1% of spending in 24 states.[19]
The Reality of Medicaid Waivers
Medicaid waivers were originally intended to test innovative methods of payment; but small-scale §1115 demonstration projects are now rare. Instead, waivers are now the primary method of financing the comprehensive delivery of Medicaid services and distributing funds to states.
Demonstration waivers still require formal evaluations, but the process has never been rigorously scientific. Evaluations are methodologically slipshod and pro forma; they usually do not identify appropriate counterfactuals, quantify costs, establish a well-constructed control group, or fully assess what had previously been promised.[20] Projects are also selected for political reasons rather than being randomly assigned.[21] Even if evaluations were rigorous, their use would be limited because they are not undertaken until the waiver term is completed—by which time it has typically already been renewed.
The availability of federal matching funds (worth up to $9 for each $1 that states spend) makes expenditure on Medicaid, relative to spending on other policy priorities, potentially lucrative. To prevent states from exploiting this, the availability of matching funds has historically been constrained by limits on covered benefits and eligibility requirements. But, as the Government Accountability Office (GAO) notes, waivers allow states to turn “what otherwise would not be considered an allowed Medicaid cost into a covered Medicaid cost.”[22]
The Medicaid and CHIP Payment and Access Commission estimated that only 6% of §1115 Medicaid waiver expenditure (about 3% of total Medicaid spending) in 2019 was spent on services and populations for which states would otherwise not be able to claim federal matching funds.[23] But waivers also allow states to inflate the amount of federal funding that they claim for services that do fall within the traditional scope of the program. Waivers have also facilitated the incremental expansion of the program, by establishing staging posts for subsequent statutory expansions.
Budget Neutrality
HHS’s “budget neutrality” requirement for §1115 waivers—which is meant to ensure that they do not increase costs to federal taxpayers—is not clearly defined, supported by appropriate evidence, or well enforced.
Budget neutrality is a standard established by the White House Office of Management and Budget, rather than a statutory requirement—and its terms have tended to shift with the change of administrations. Waiver payments to states are often based on inflated benchmarks, which owe more to political negotiations with states than to data analysis.[24] Once funding terms are set, states typically supply a hypothetical baseline counterfactual level of Medicaid costs, which HHS must largely accept on faith.
But this faith is misplaced: investigations have shown that states routinely attempt to inflate federal funding with accounting sleight of hand. In some cases, states increase Medicaid program costs prior to claiming waivers, in order to drive up baselines to which they become entitled. And in other cases, the baseline costs are purely fictional. HHS paid Texas according to a benchmark based on hypothetical maximum Medicaid fees that the state did not actually pay providers.[25] Various states count soon-to-be-released prisoners as hypothetical Medicaid beneficiaries, for the purpose of establishing a baseline of expenditure on them, against which “savings” can be claimed. Other states have “made illusory Medicaid payments to government-owned providers” to inflate hospital costs, and then claimed savings against them.[26]
HHS has often been highly accommodating to state preferences—routinely allowing them to establish alternative baselines with questionable estimation methods, often without requiring justification for deviation from standard practice. States are frequently permitted to count costs that weren’t incurred, use outdated data, carry forward savings for reuse over several years, or manipulate the five-year waiver time window to exclude expenses from savings calculations.[27] As states roll over savings from year to year, while authorization periods often overlap, it is often unclear which costs and savings are associated with a given waiver.
Even when benchmarks are clearly specified, they are often poorly enforced. Reporting of expenditures is inconsistent and inadequate.[28] HHS has increasingly afforded states flexibility to make midcourse “corrections” to budget-neutrality targets if their expenditures overshoot.[29] This generally occurs without Congress or oversight agencies being informed, so all the pressure and information comes only from the state. Such ad hoc adjustments are guided by political calculations and constrained by few rules.
There is not even any robust enforcement mechanism in cases where states clearly have claimed excess funds. States do not wait for “savings” to truly accrue before spending them. By the time that payment errors are calculated, surplus allocations have already been spent—and there is neither an effective mechanism nor the political will to claw back funds. State and federal administrations will often have changed in the interim. Even states that have violated explicit provisions have escaped without sanctions, and they are often allowed to keep savings to which they are not entitled.[30]
Of five demonstrations assessed by GAO in 2013, spending limits under the criteria specified by HHS would have been $33 billion lower than the level of spending that was actually approved, implying overpayment by 16%.[31] Waivers for newly established beneficiary groups are particularly vulnerable to speculative baselines. GAO estimated that Medicaid payments to Arizona under its comprehensive waiver exceeded the appropriate counterfactual benchmark (the level of spending that would have occurred in the absence of a waiver) by 57%.[32]
In the absence of precise waiver approval criteria, politics often fills the void, with different rules seemingly applying to different states on the basis of partisan political calculation by HHS.[33] The waiver process neutralizes scrutiny by enlisting states to make requests, giving governors credit-claiming opportunities with federal money and providing presidents with discretionary resources that can be used to reward friends and punish enemies.[34] In general, it allows presidents and governors to sidestep Congress and institutional fiscal constraints embedded in the legislative process.
Although waiver arrangements limit federal funding for states in a method similar to per-capita caps, the voluntary nature of the arrangement allows states to participate only when they believe that it allows them to get more money from the federal government.
Waivers serve as a one-way ratchet to grow Medicaid spending. Unlike “shared savings” arrangements, waivers require that states spend all the “savings” that are generated. As a result, they eliminate any incentive that states might have to reduce Medicaid expenditures in a way that reduces the program’s costs to federal taxpayers.
Eligibility Expansions
Waivers of Medicaid’s eligibility requirements are often justified with vague claims that steering funds away from the program’s intended beneficiaries will further “the objectives” of the program.
In the early 2000s, HHS used §1115 waiver authority to divert funds from the Children’s Health Insurance Program to cover parents, despite the lack of statutory authority for covering childless adults, by citing a supposed spillover effect on the health of children, for which there was no evidence.[35] Similarly, it was claimed that allowing states to divert Medicaid funds to pay for prescription drugs for seniors with incomes above Medicaid’s income-eligibility cutoff would reduce the program’s costs.[36]
Prior to the 2010 ACA, §1115 waivers were the only way for states to expand Medicaid coverage to able-bodied childless adults. The George W. Bush administration encouraged states to request waivers that would allow them to claim federal funds to expand private insurance coverage, including employer-sponsored plans.[37] Indiana used waivers to redirect Medicaid Disproportionate Share Hospital subsidies into health savings account payments for low-income individuals.[38] Medicaid waivers formed the foundation of Massachusetts’s 2006 health-care reforms, which served as a prototype for ACA.[39]
By subjecting Medicaid to extensive “essential health benefit” regulations, ACA greatly reduced the degree to which Medicaid waivers can be used to implement substantially cost-reducing innovations. But the appeal of waivers to states has not been diminished. The Supreme Court ruled that Congress could not compel states to expand Medicaid to newly eligible beneficiaries, so the expansion of the program has become more of a matter of ad hoc negotiation. As the Obama administration was desperate to secure their participation, states had much leverage to obtain waivers on favorable terms.[40]
Arkansas obtained a waiver for a “private option” Medicaid expansion, which allowed it to claim federal reimbursement at 167% of its standard Medicaid payment rates to medical providers.[41] Other late-expansion states sought to use waivers to maximize revenues from various federal programs available for low-income adults. For instance, Georgia requested a waiver to reduce the Medicaid expansion eligibility limit from 133% to 100% of the federal poverty level, knowing that fully federally funded exchange subsidies would be available to beneficiaries with incomes above 100% of the poverty level—raising the federal share of subsidies from the 90% provided for Medicaid beneficiaries to the 100% provided under the exchange.[42]
States have also claimed Delivery System Reform Incentive Payment (DSRIP) §1115 waivers to give safety-net hospitals the discretion to use Medicaid funds to promote holistic “population health,” rather than being limited to a narrow quid-pro-quo relationship between payments and the delivery of specific services.[43] As a result, states have claimed funding for vaguely defined extraneous purposes, which are largely untraceable and inherently unaccountable. Waiver agreements often fail to specify precisely what funds will be spent on, and New York has seen DSRIP dollars steered to highly profitable hospitals that happen to be major political donors employing high-cost consultants.[44] California and Texas have largely reserved DSRIP funds for public hospitals, where funds are typically captured for state fiscal purposes—allowing them to use Medicaid to draw federal revenue without expanding access to medical care.[45]
Extraneous Expenditures
The openhanded nature of federal funding for Medicaid has made states eager to use waiver funds to finance their other responsibilities.
More recently, some states have invoked theories of “social determinants of health” to get waivers entitling them to use federal Medicaid matching funds for social services such as public health, workplace training, and housing programs.[46] In total, 19 broad “social determinant of health” waivers had been approved as of January 2024, with 16 more pending.[47]
For example, North Carolina employed a “Healthy Opportunities” waiver to claim federal Medicaid funds to remedy “housing instability, transportation instability, interpersonal violence, and toxic stress.” Its services range from meal delivery to the housebound, home renovations for children suffering from asthma, and legal support to victims of domestic abuse.[48] Arkansas, Arizona, Massachusetts, and Oregon have similarly received waivers to address “food insecurity” or “housing instability,” while Florida, Hawaii, and Illinois use Medicaid funds to support housing for those with serious mental illness and substance abuse disorders.[49]
Waiver funds are often distributed through private “nonprofit” organizations, such as one led by former secretary of education Arne Duncan in Illinois, which is looking to claim federal Medicaid funds to pay for community-based programs to stop gun violence. California, Colorado, Connecticut, Maryland, New York, and Oregon are also seeking approval of Medicaid funds for similar gun-violence-prevention programs.[50]
Although federal law prohibits the use of Medicaid funds to pay for abortions, California has sought Medicaid waiver funds to help its reproductive health clinics treat an increased number of visitors following the Dobbs v. Jackson ruling (which allowed other states to restrict abortion).[51] California claims that waiver dollars would not be used to directly pay for abortions but rather that they would free up “state-only” funds for the purpose.[52]
GAO notes that waiver expenditures are now sometimes “only tangentially related to health coverage for low-income individuals,” while broad grants are frequently duplicative of other federal and grant programs that are already available.[53] States can “double-dip” by using other federal funds to pay the state share of Medicaid matching contributions. Incidental “social determinant” health impacts are therefore increasingly used by states to turn Medicaid into an open-ended source of matching funds for social services, circumventing spending limits on other grant programs expressly designated by Congress.
HHS officials have resisted specifying formal rules that would reduce their discretion in approving Medicaid waivers.[54] The department has not issued any specific criteria defining what types of waiver expenditures would legitimately further “the objectives” of the Medicaid program, as required by statute.[55]
Reform Considerations
Because 75% of Medicaid spending is governed by §1115 or §1915 waivers, no reform could ensure that Medicaid as a whole is cost-effective and aligned with congressional priorities if it doesn’t touch waiver spending.
Indeed, waivers affect even the remaining 25% of Medicaid spending because the very existence of waivers influences the character of the program’s other expenditures. For instance, states may opt against cutting Medicaid costs if it allows them to receive higher payments from the federal government under waivers in the future.
Waivers were intended to improve cost-effectiveness in the purchase of medical services for the Medicaid program. But because they provide no incentive for states to reduce the program’s overall expenditures, they have not done anything to save money for federal taxpayers. Rather, they have served as a one-way ratchet for increased Medicaid costs.
Federal appropriations are a catalog of congressional intent for expenditure. Every year, Congress enacts trillions of dollars of spending, either directly or through grants to states, specifying detailed constraints and conditions on how funds may or may not be used. But HHS has increasingly allowed states to use Medicaid waivers to circumvent these restrictions, so that federal funds may be claimed for all kinds of extraneous purposes that would normally require expressed congressional approval. The result has been the opportunistic expansion and inequitable sprawl of Medicaid spending beyond the program’s core purposes, with little accountability or deliberate control by Congress.[56]
Most states have grown accustomed to receiving Medicaid expenditures to which they should not be entitled under any reasonable definition of the program’s intent. Furthermore, these windfalls are not distributed in anything like an equitable or cost-effective manner. The immediate transition to a set of well-enforced Medicaid waiver rules would imply substantial cuts in funding for many states—and thus would likely fail in the face of fierce political pushback.
The overextension of Medicaid waivers also cannot be solved by a simple prohibition on the use of waiver funds for nonmedical purposes. Some nonmedical spending—such as Long-Term Services and Supports (LTSS) for basic activities of daily living—are important, central, and legitimate ends of the Medicaid program.[57] In any case, funding for such purposes is not distinct from medical funding; waivers are often employed to fund LTSS, under the justification that it will forestall costly hospitalizations, so funding for medical and nonmedical services is often jumbled together.
Attempting to check inappropriate claims for federal funds through Medicaid waivers by prohibiting their use for specific undesired purposes would likely lead to a game of Whac-A-Mole, which states could easily circumvent by employing indirect financing schemes such as supplemental payments and mandates on managed-care organizations.
Similarly, effective reform cannot be achieved simply by increasing the specificity and enforcement of the program’s budgetary rules. Medicaid waiver expenditures increasingly involve a web of elaborate financing mechanisms, such as managed care, population-based payments, and supplemental funds for providers, which are not directly tied to the provision of specific services for beneficiaries. It is therefore often not possible to identify an objective counterfactual level of expenditures for specific narrowly defined purposes. The problem is exacerbated by the uncertainty that the business cycle imposes on Medicaid’s caseload. In the real world, where states are attempting to manipulate funding windows, cost structures, and scope-of-waiver applications to inflate the benchmarks for federal funding to which they are entitled, waiver claims are practically impossible to police with more detailed regulation.
The more narrowly tied a waiver is to specific benefits or beneficiary groups, the harder it is to determine a counterfactual level of cost—because of the debatable scope of the waiver and the prospect that states might be able to manipulate which expenses are counted as associated with the demonstration. The narrower the scope of a waiver, the less likely it is that HHS will be able to objectively determine an objective counterfactual by which its cost may be assessed.
This is fortuitous because the day of the narrow demonstration waiver advanced by states under good faith for genuinely experimental purposes is gone—if it ever existed. The time and expense involved in waiver applications mean that Medicaid is already moving toward comprehensive waivers, aggregating all kinds of Medicaid expenditures and payment reforms in single funding applications. What good does it do to have multiple waiver benchmarks, with ill-defined boundaries, over different time horizons in the same grant program between the states and federal government—other than to invite fiscal chicanery?
Reform Proposal
The problem with Medicaid waivers is that they can be manipulated to inflate the total level of federal funding claimed by each state. This can be solved by capping the total level of federal funding that each state opting for waivers may claim from the federal budget, for all waiver and non-waiver expenditure alike.
Proposal: States adopting Medicaid waivers should be subject to a single overall cap on federal Medicaid funding.
This policy should preferably be enacted through legislation—but if that is not possible, it could be done by executive action that makes the cap a principle and condition of waiver approval.
A single unified spending cap for each state, applying to all Medicaid expenditures, would eliminate the ability of states to manipulate Medicaid benchmarks and the federal funding that they receive by selectively shifting costs in and out of waiver programs—by altering the scope of services subject to the waiver, the set of beneficiaries subject to them, or the time window in which expenditures are to be assessed.
A single cap would also eliminate the huge administrative expense and rigidity that the federal bureaucracy must impose on states in a futile attempt to police and evaluate multiple narrow waivers. So long as states comply with aggregate spending caps, the reauthorization of existing well-functioning waiver arrangements would be simpler, and future waiver approvals will be less politicized. Given the sweeping scale of Medicaid waivers, establishing this cap would also better focus the program on the neediest beneficiaries.[58]
Caps could be designed in various ways. For example, they could be set to limit the growth of total federal Medicaid funding per beneficiary, as proposed by the American Health Care Act, which passed the House of Representatives in 2017.[59] That legislation proposed to limit the rate of increase of federal matching aid, which each state could claim, in line with the rate of inflation in the health-care sector. Alternatively, caps in federal funding could be based on the cost of delivering services that states are required to provide to low-income residents.[60] Such caps could be based on the prices that Medicare pays for medical services, adjusted for utilization trends, or based on what other similar states spent on mandatory Medicaid benefits.
The respective merits of these approaches depend on a host of economic, political, and technical considerations; each has advantages and disadvantages. Because the desirable level of total Medicaid spending is a matter of dispute, and the counterfactual level of matchable Medicaid spending in the absence of a waiver is not exogenously fixed, all methods proposed for setting caps are, to some extent, arbitrary. The problem with waiver baselines is not that they are objectively “incorrect” with respect to any ideal level of federal aid to states. But waivers as they exist now, with a variable scope, allow states to increase the level of funding associated with them. The approach of using budget neutrality as the primary method of limiting spending under Medicaid waivers is also inherently flawed because the baseline level of state spending is a moving target that is also under state control.
Either of the aforementioned cap methods would be effective in curtailing the abuse of Medicaid waivers because proposed limits on payments to states would be set by the federal government, independent of the design of state Medicaid programs—and therefore not reliant on them for providing information about highly idiosyncratic costs. In contrast to current arrangements, states would no longer be able to establish, design, and structure waivers to alter the amount of federal aid that they can receive. Instead, the cap would be set by the federal government, based on national data on medical costs, utilization, and eligibility, and by comparing trends across states.
It is not possible to effectively prevent the abuse of Medicaid waivers solely by limiting expenditures that states opt to categorize under waivers; limits must also apply to claims for federal matching funds that states selectively leave out of them.
Acknowledgments
The author would like to thank Seth Gold, Josh Trent, Stuart Portman, Nina Owcharenko Schaefer, Dennis Smith, Theo Merkel, Gavin Proffitt, Michelle Rosenberg, Susan Barnidge, Catina Latham, and Peter Mangano for their input.
About the Author
Christopher Pope is a senior fellow at the Manhattan Institute. Previously, he was director of policy research at West Health, a nonprofit medical research organization; health-policy fellow at the U.S. House Committee on Energy and Commerce; and research manager at the American Enterprise Institute. Pope’s research focuses on health-care payment policy, and he has recently published reports on hospital-market regulation, entitlement design, and insurance-market reform. His work has appeared in, among others, the Wall Street Journal, Health Affairs, U.S. News & World Report, and Politico.
Endnotes
Photo: LPETTET/iStock/Getty Images Plus
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).