Mental Health Courts in an Era of Criminal Justice Reform

Photo by Darrin Klimek/Getty Images
Introduction
Mental health courts place seriously mentally ill defendants in community treatment as an alternative to incarceration. In recent decades, these and other “problem-solving” courts have expanded dramatically nationwide. These programs were long seen as core elements of criminal justice reform and frequently reduce recidivism more effectively than traditional court systems.
But recently, problem-solving courts’ place in the criminal justice reform agenda has become more ambiguous. Not only has energy shifted toward more radical ideas (such as jail “abolition”), but some far-reaching reforms threaten court programs’ traditional incentive structure. Mental health courts rely on criminal sanctions as leverage; they lose that leverage when criminal justice reforms reduce or jettison the use of criminal sanctions entirely.
This brief assesses mental health courts’ future in an era of criminal justice reform. It considers how sentencing, bail, and discovery reforms threaten the structure of mental health courts. It also evaluates attempts to “co-opt” the model, through New York’s “Treatment Not Jail Act.”
Overall, the brief argues that mental health courts will retain their relevance for the foreseeable future, owing mainly to their small scale. Mental health courts serve only a small fraction of the universe of mentally ill offenders. They will therefore never contribute significantly to mass de-carceration, the goal of progressive reformers. But that also means that they are likely to retain their relevance, even if the use of criminal sanctions declines, as long as the population of mentally ill offenders remains substantial.
This brief will conclude with suggestions on how to sustain mental health courts in the future.
Problem-Solving Justice
Participation in a mental health court program begins when someone charged with a crime is identified as seriously mentally ill. Instead of being sent through the standard criminal court process, he enters mental health court, acting on the advice of his attorney and with the participant’s full consent. There, the judge, prosecutor, defense attorney, and court staff monitor his compliance with a community-based treatment program that may include regular court check-ins, attendance at group therapy, drug testing, and medication compliance. Program lengths vary, but 18 months is standard. Upon completion of the program, the participant may see his charges reduced or dismissed, and he will avoid incarceration, which would otherwise be justified by conviction for the charges that initially brought him to the court’s attention.
Mental health courts are a species of the genus “specialty courts,” “specialty dockets,” “therapeutic courts,” “treatment courts,” “accountability courts,” or “problem-solving courts.” Problem-solving courts were developed in the latter decades of the 20th century, as a reaction to “assembly line justice.” In the late 1980s, court systems were overwhelmed by the sheer number of charges and defendants. Judges administered a system that resembled a factory in that the overwhelming majority of cases were resolved, via plea, with cursory attention given to the reasons that defendants offended or whether defendants benefited from the court experience.[1]
The first notable problem-solving courts were the Miami-Dade drug court (1989) and the Midtown Community Court in New York City (1993). The first true mental health court was also South Florida–based, in Broward County in 1997. Problem-solving courts are also called “specialized dockets” because all participants share some feature in common, such as an addiction, a diagnosis of serious mental illness, or a compulsive tendency toward low-level offending. The specialized docket allows court professionals to develop expertise and concentrate more on the “root causes” of crime than is the case with a standard criminal court.
Problem-solving courts embrace plea-based adjudication. Plea-based adjudication has been criticized for undermining the adversarial dynamic that some view as a crucial guarantee of defendants’ rights.[2] By contrast, problem-solving courts, and mental health courts in particular, see non-adversarial procedures as beneficial and emphasize “collaboration”[3] among the judge, defense attorney, prosecutor, court staff, and social services professionals.[4] Strong emphasis is also placed on developing a personal relationship between participants and the judge through regular check-ins, conversations about life’s challenges beyond legal issues and treatment, and graduation ceremonies.[5] That relationship is enabled by the fact that mental health courts tend to be small in scale: more than 100 participants at one time would be considered a large program, meriting very close oversight of operation.[6]
Mental health and other problem-solving courts are all, in a sense, “community” courts. Judges and other court staff rely heavily on community-based mental health service providers. The relationships developed with providers are essential to courts’ functioning because the court programs themselves generally do not control their own dedicated resources. Housing, therapy, drug testing, and other components of a treatment plan are essential to mental health courts’ functioning, but program participants access them mainly through the ministrations of court staff. Courts “facilitate” access to those resources; for the most part, they do not directly provide them.[7]
Mental Health Courts: Theory and Practice
Mental health courts have spread from “only a few” in the late 1990s to about 650 today.[8] (There are about 1,800 drug courts.)[9] The rapid spread of mental health courts shows the motivation for innovation and reform coming from actors within the American criminal justice system—as opposed to legal and fiscal pressures exerted from outside the system. In fact, judges have been the driving force behind mental health courts’ expansion, and several individual judges built high-profile reputations from this reform, such as Steven Leifman,[10] Matthew D’Emic, Ginger Lerner-Wren,[11] and Evelyn Lundberg Stratton.[12]
To promote adherence to treatment, and therefore avoid recidivism, mental health courts use the threat of incarceration. They are technically voluntary but are best seen as part of a “continuum of coercive care” through which the government works to reduce the rate of untreated serious mental illness. Involuntary hospitalization and assisted outpatient commitment both use coercion in a more straightforward form than mental health courts, in which, as noted, participant consent is always required. Inpatient and outpatient commitment are also civil procedures that do not involve the threat of incarceration. Many people with behavioral health disorders are not actively seeking treatment. A well-structured behavioral system will therefore utilize a few different forms of coercive care, in order to serve different kinds of mental disorders and even the same individual at different stages of recovery.
Structurally, mental health courts use both carrots and sticks (“leveraged treatment”).[13] But their spirit is more carrot than stick.[14] The expansion of drug and mental health treatment courts was a core element of the criminal justice reform movement of the 2000s and 2010s, a bipartisan push whose overall goal was to reduce incarceration.[15] The presiding judge has the discretion to assess whether a program infraction, such as a positive drug test, merits sanctions or expulsion.[16] Sanctions could include less freedom (more frequent drug testing and check-ins) and extended time in the program. Mental health courts often boast high graduation rates,[17] which reflects program leaders’ willingness to “work with” participants over infractions instead of expelling them. They are considered more flexible programs than standard probation, the most common form of community supervision, out of which mentally ill individuals fail at disproportionately high rates.[18] Standard probation, for all offenders, has declined as mental health courts have expanded.[19]
Mentally ill defendants are overrepresented throughout the criminal justice system.[20] A 2011 study estimated that 1 million are under community or correctional supervision.[21] Other research has estimated that about one-third of seriously mentally ill Americans will have some contact with the criminal justice system in their lifetime.[22] This extensive involvement has prompted governments across the nation to develop various programs, based in public safety agencies, to divert or serve seriously mentally ill offenders.[23] Mental health courts are the court-based node.
Mental health courts serve only a segment of the mentally ill offender population. They do not enroll defendants who are too mentally unfit to stand trial, found “not guilty for reason of insanity,” or who have been accused of a mass shooting. However, many professionals involved in specialized treatment courts, such as those affiliated with the organization All Rise, argue that “high-risk, high-need” offenders are the most appropriate population for mental health courts to serve.[24] A first-time offender facing a nonviolent misdemeanor charge diagnosed with a mild mental disorder would be seen, by much of the public, as a prime candidate for some form of diversion. But treatment court professionals would not see him as a prime candidate for mental health court. Not only do lower-level charges lack the leverage of the incarceration threat requisite for mental health courts’ functioning, but lower-level charges do not merit 18 months of intensive supervision.[25] A first-time offender charged with a low-level misdemeanor, acting on the advice of his attorney, would likely be able to find a better “deal” than 18 months of regular court checking, regular attendance at group therapy, drug testing, and medication compliance. The problems in the lives of mentally ill offenders developed over many years. If they are to be addressed at all, they will require a treatment program (“dose”) of sufficient duration and intensity. For effective treatment, the length of the program, not just the “stick” effect of threatened incarceration, is requisite, though both are a function of the seriousness of the charge.
Over time, mental health courts have become more comfortable dealing with individuals with more felony and even violent charges.[26] Programs are not always free to decide which charges to work with, as charge seriousness can sometimes be a function of grant stipulations.[27] Prosecutors must consent, as victims often must, when relevant (though lack of victim consent can sometimes be overruled).[28]
Do Mental Health Courts Work?
Assessing whether mental health courts work largely comes down to whether someone seriously mentally ill and charged with a crime is less likely to reoffend having participated in a mental health court than were he sent through the standard criminal court process (“treatment as usual”). The quasi-experimental conditions favored by social scientists are not easy to establish for mental health courts.[29] Participation is not assigned on a lottery-style or random basis. In a given community, seriously mentally ill offenders who do not participate in mental health court broadly differ from those who do, in terms of their charges and clinical acuity. Therefore, it cannot be assumed that everyone who does not go through the program would have had the same experience as everyone who has. Furthermore, any evaluation of one mental health court program cannot be assumed to apply definitively to the universe of programs.[30]
Some programs enroll 10–15 participants; some 100–200. Some deal only with misdemeanors, others only felonies, others a mix. Some do not work with people charged with violent charges; others will. Programs vary in the kinds of “serious mental illness” participants have.[31] Some are based in rural areas with sparse community mental health service offerings; some are based in urban areas with a stronger concentration of psychiatrists, therapists, etc. Many programs do not even maintain the kind of data that would allow for a proper evaluation, and those who do maintain that data often do not post charge and acuity information online.[32]
Though, in principle, many outcome metrics could be measured for problem-solving courts,[33] recidivism is the most standard quality metric. Recidivism plagues the criminal justice system generally.[34] Mentally ill offenders recidivate at higher rates than offenders without mental illnesses.[35]
Two recent surveys of the relevant literature found that mental health courts had a modestly positive effect on recidivism, compared with the standard criminal court process.[36] The most reliable estimate would be that participants are 20%–40% less likely to recidivate as a result of going through mental health court than going through normal criminal court.[37] Evaluations of mental health court programs in New York have placed them in this same range of effectiveness.[38]
As a general proposition, people with untreated serious mental illness are more likely to commit crimes than people with serious mental illness who are in treatment.[39] But whether it is the treatment itself that causes mental health court program participants to re-offend less would have to be established via a thorough evaluation of improvements in participants’ mental health symptomology. An alternative theory posits that the more important “dose” supplied by mental health court interventions is the close supervision and relationship with the judge.[40] Some studies have found that participation in a mental health court improves symptoms and makes mentally ill individuals more engaged in services.[41] But results have varied.[42] Surely, the quality of the treatment services must matter; the quality, in turn, will differ among different court programs.
Mental Health Courts and Criminal Justice Reform
Establishing and expanding mental health and other problem-solving courts was initially a top priority of the criminal justice reform movement. But additional changes prioritized by criminal justice reformers are threatening mental health courts and the good that they appear to do. Any attempt to reclassify crimes to make them less “jailable” will also make those same charges less appropriate for mental health court.[43] This is clear from the experience of drug courts. When Oregon decriminalized hard drugs (Measure 110 in 2020), demand declined for drug court programs. One highly regarded program, Multnomah County’s Sanction Treatment Opportunity Progress Court, closed entirely.[44] In California, demand for drug courts declined in the wake of Proposition 47 (2014), which reclassified some formerly felony charges as misdemeanors.[45]
New York City is host to an ambitious criminal justice reform movement. Its achievements, throughout the 2010s and 2020s, could have affected the structure and dynamics of mental health courts. Bail reform, which passed in 2019, was justified as a way to weaken prosecutors’ leverage in plea-bargaining. Defendants held on bail are often said to be susceptible to “bad deals” urged on them by prosecutors who, allegedly, take advantage of defendants’ motivation to exit correctional custody as quickly as possible.[46] One such “bad deal” could conceivably be 18 months of intensive supervision in a mental health court. Additionally, the rate at which criminal cases are being prosecuted or resulting in convictions has fallen as a result of local district attorneys’ “decline to prosecute” policies and the compliance burden of discovery reform.[47] This, in turn, reduced the leverage to push defendants into treatment, since there is a higher chance that their cases will simply get tossed anyway. As a question of best practices, experts advise mental health and other treatment courts to place participants in their program in a “timely” manner, so that treatment can begin as soon as possible after arrest.[48] Discovery reform makes that standard harder to meet. Instead of promptly resolving charges via a plea to enter mental health court, public defenders urge their clients to first determine whether prosecutors comply with discovery reform’s evidence-gathering requirements in a timely fashion. A 2023 Albany Times-Union analysis found that, in the wake of bail and discovery reform, participation in drug courts in New York City fell by more than 80%.[49]
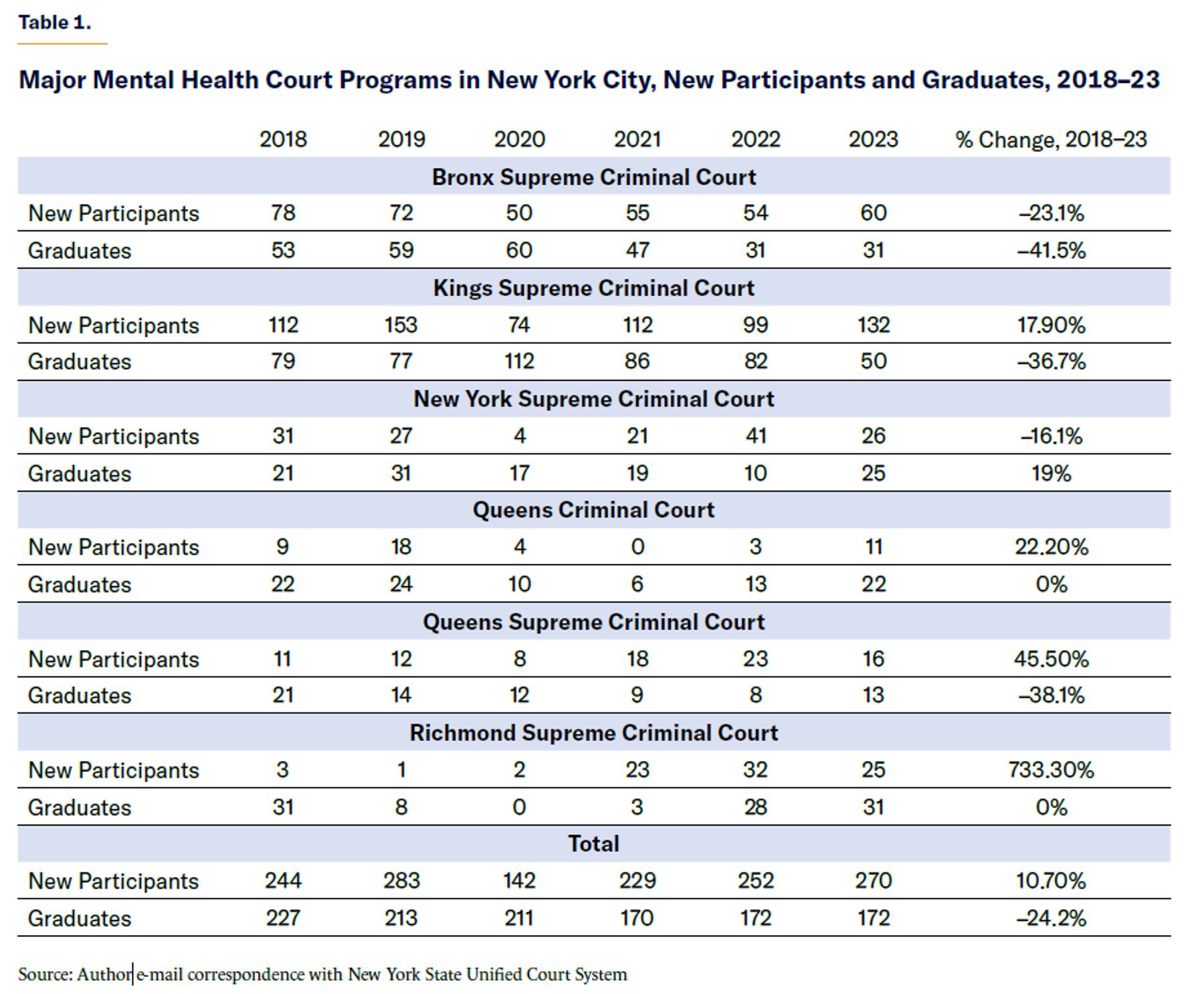
Table 1 presents data on major mental health court programs in NYC. Covid disruptions aside, some programs have experienced a decline in new participants, others a modest increase. It is difficult to articulate a clear trend.
A few factors could explain why mental health courts may enjoy continued relevance in an era of criminal justice reform. First, leading New York Democrats, including prosecutors’ offices, remain supportive and have even advocated for expanded use of mental health courts.[50] In the current (FY25) fiscal year, New York State will spend $24.7 million on problem-solving courts, a program that received a $9.3 million increase during the last budget cycle. The funding boost will add an additional 100 full-time employees for mental health courts, of which there are 42 in NYS.[51] Second, as mental health courts have matured, staff have grown more accustomed to enrolling participants with more serious charges. If defendants charged with less serious felonies are now able to get “better deals,” mental health courts may, in effect, replace them with more dangerous defendants who in previous eras would not have been enrolled. Higher-risk cases merit closer monitoring[52] because they pose a greater risk to public safety. Expansion into harder cases may therefore have to come at the expense of expanding the raw quantity of participants. Third, increased crime: after declining in the 2010s, in 2022 and 2023, the amount of “serious” (seven major felonies) crime in NYC stood at about the level of the mid-2000s, where it was before many of the major criminal justice reform initiatives went into effect.[53] As long as there is no shortage of crime committed by seriously mentally ill New Yorkers (tens of thousands of whom receive no treatment),[54] mental health courts will not lack demand for their services.
The criminal justice reform movement of the 2000s and 2010s, which prioritized problem-solving courts, had a bipartisan cast.[55] The criminal justice movement in the 2020s is less bipartisan. Progressives play more of a leading role, especially in blue states. Progressives are also more ambivalent about problem-solving courts. They have accused programs of “net-widening” (expanding the criminal justice system’s reach beyond candidates for incarceration), criticized programs’ combination of treatment and punishment as unstable and inevitably favoring the latter,[56] and charged that mental health courts’ non-adversarial style compromises defendants’ rights.[57] Mental health courts can result in incarceration.[58] If avoiding incarceration at all costs is the bottom line definition of “criminal justice reform,” as it is for many progressives, then a program that uses the threat of incarceration will not fit perfectly within the overall criminal justice agenda. A criminal justice culture that embraces ideas such as “making diversion the norm” and “for some people who get arrested, the best response is nothing—no criminal justice engagement at all” may eventually question whether even mental health courts’ requirements are too onerous for participants to fulfill.[59]
Another risk to the functioning of mental health courts is co-option into a broader program that they are not equipped to handle. A top priority of New York’s criminal justice reform community, since 2020, has been the passage of “Treatment Not Jail,”[60] which would require every county in NYS to operate a mental health court, require consideration for eligibility for any individual accused of a felony or misdemeanor, strip prosecutors’ authority over determining eligibility, and eliminate guilty pleas as a requirement for participation.
Proponents of this legislation argue that its goal is expanded access to mental health and other treatment courts. But the details are more complicated. Treatment Not Jail poses multiple threats to the traditional mental health court model. First, without the ability to require guilty pleas, the program’s leverage to encourage participation in treatment will be sharply reduced. Second, there are legitimate reasons to restrict access to any mental health program because some people, depending on their acuity or dangerousness, require a higher level of care. There are many examples of serious, and even heinous, crimes committed by mental health court participants and graduates.[61] Treatment Not Jail would both authorize far more serious charges and weaken the authority of prosecutors,[62] the stakeholder most likely to bar access based on dangerousness. Third, with respect to existing programs, such as those in NYC, creating new mental health courts with less stringent requirements could create competitor programs that would be more attractive to many, perhaps most, similarly situated defendants and therefore undermine existing programs’ enrollment.
New York is already host to an extensive array of pure diversion programs.[63] A mental health court that does not require a plea, and for which prosecutorial involvement is almost pro format, would not be as distinct from mainstream diversion programs as the more traditional felony mental health court programs that exist in New York.
Creating programs in jurisdictions that do not have them and pursuing ways to ensure that more people benefit are both appropriate goals. But the main limitation on program expansion—and one would expect progressives to understand this—is dedicated resources.[64] To thrive in a mental health court, participants need access to court staff who are not overwhelmed by unrealistic caseloads and access to housing and therapy. Outside the context of problem-solving courts, transitional housing has been systematically underfunded as housing programs have shifted their emphasis toward permanent housing.[65] That would have to be confronted to support a more responsible expansion.
Cognizant that expanding mental health courts will entail taking more risks with violent offenders, Treatment Not Jail proponents emphasize that many consider mental health courts even more effective with that cohort than for those charged with misdemeanors.[66] As noted earlier, the model is arguably more appropriate for “high-risk” individuals, whose charges are serious enough to merit incarceration and 18 months in community supervision. But saying that a mental health court participant is less likely to recidivate than a mentally ill defendant who is sent through the standard criminal court process is different from saying that the former will never recidivate. Mentally ill people who go through the standard criminal court process recidivate at very high rates. Therefore, that is a low baseline for an “evidence-based” program to exceed.
Mental health courts do not cut recidivism to zero. And measures of “recidivism” do not always account for the total amount of crime committed (as distinct from how many people commit at least one crime) and the seriousness of the crime. “Reoffend” could mean something different in the case of someone charged with a violent felony crime, compared with someone charged with a nonviolent misdemeanor. A full calculation of whether mental health courts “work” would have to factor that difference into a cost-benefit analysis. From a community perspective, a small handful of violent crimes committed by mental health court participants could heavily outweigh, and even offset, the benefits experienced by other participants. It is a near-certainty that, in absolute terms, the more violent felony participants that mental health courts enroll, the more violent crime will be committed by mental health court participants. Traditionally, mental health courts aimed at “increas[ing] public safety,”[67] not just reducing the use of incarceration.
Conclusion: Quality and Quantity
Even if the evidence supporting mental health court programs is mixed, they are promising enough to protect from ill-advised reforms, such as Treatment Not Jail, that would undermine them. To make the most out of the model, policymakers must be concerned about both quantity and quality.
Quantity: Expand mental health courts to communities without them.
The most promising communities for expansion are those still without programs. Communities that still do not have a mental health court by now are likely not deep blue and thus not host to an ambitious criminal justice reform movement; or not affluent, making support from state government probably critical.
Communities with mature programs are in a different situation. They likely developed their mental health court during a previous wave of criminal justice reform. In these communities, existing mental health court programs may now be doing all the de-carcerating that they will ever be capable of doing. Communities with mature programs are therefore in a position wherein the conservatives must now defend the achievements of past generations’ progressives against progressives on the current scene.
Quality: Ensure that programs operate at an appropriate scale, place participants promptly, and evaluate programs experiencing leadership transitions.
Mental health court programs now 15–20 years old may soon see founding judges retire. Mental health court judges have wide power to assess the seriousness of infractions and eligibility and must be able to develop constructive personal relationships with participants. A program that researchers evaluate as successful cannot be assumed to be equally successful under an entirely new leadership team working in an entirely new criminal justice context. Thus, mental health courts’ leadership transition will necessitate ongoing evaluation, even of programs widely considered effective.
Scale and timely placement are related concerns.
Big-city jurisdictions with mature programs also often face housing shortages. To succeed in mental health court, participants need housing stability, meaning placement in a residential program. In NYC, a shortage of slots in residential programs is often cited as a barrier to expansion.[68] Someone can still be placed in mental health court if no housing is immediately available to him, but he may need to wait weeks or even months, in jail, to begin the program in earnest, thus frustrating the goal of “timely” placement.
The longer mental illness goes untreated, the greater the risk of further deterioration—hence the value of timely placement. As noted earlier, “reforms” designed to weaken prosecutorial leverage, such as discovery reform, will make it harder to place participants in treatment in a timely manner, as participants and their lawyers will spend time weighing other options.
Mental health courts, relative to the universe of mental illness–related offending, are small-scale programs, and should remain so. Their small scale offers lessons to both sides of the criminal justice debate. Progressives cannot use them as a tool for mass de-carceration. Conservatives should recognize that they may still function amid other criminal justice reforms, so long as there are enough mentally ill offenders who would benefit from them.
Mental health courts’ expansion indicates broad support, in New York and across the nation, for reducing incarceration, especially with respect to the mentally ill. Mental health courts, in NYC, are thus far maintaining their relevance. But as the experience of other jurisdictions and some in NYS shows, no treatment court can take its relevance for granted.
Acknowledgments
The author would like to thank staff at the following programs for coordinating visits: Manhattan (Felony) Mental Health Court, Manhattan Misdemeanor Mental Health Court, Queens Mental Health Court, and the Reaching Individual Success Every Day (RISE) program in Franklin County, Ohio.
Endnotes
Please see the Endnotes in PDF
Photo by Darrin Klimek/Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).