Keeping Medicare Affordable: The Cost of Adding Services

Photo by Kameleon007/iStock
Executive Summary
Medicare spending on new procedures is the single factor most responsible for the projected surge in the national debt over the coming decades. This report outlines a path to averting this fiscal explosion without cutting existing benefits or hindering valuable medical innovation.
The federal government now spends more on Medicare every year than it does on national defense, and the cost of the program is expected to double over the coming decade. Following reforms over recent years, per-beneficiary Medicare spending on long-established medical procedures is now growing at little more than the general rate of inflation. By law, adjustments to Medicare fees for existing billing codes cannot increase the program’s overall cost; but there is no such constraint on the addition of new codes. Expansions of coverage are made almost entirely without consideration of (or even efforts to quantify) the additional costs to taxpayers. As a result, increases in the program’s expenditures are largely due to increased spending on new services and billing codes.
Projected economic growth will likely be sufficient to fund the current level of benefits for existing Medicare beneficiaries, as well as for those projected to retire in the coming decades. But it will not cover an open-ended commitment to pay for whatever new medical services are developed, regardless of their cost-effectiveness. To keep Medicare’s cost to a sustainable level, it is necessary to slow the addition of new procedures to the program’s basic benefits package.
To restrain the proliferation of low-value services, Congress should be required to approve expansions of Medicare’s fee schedules before they take effect. This would provide scrutiny of their additional value, relative to other budgetary priorities. Medicare Advantage can also provide additional resources to cover cost-effective services that await addition to the basic benefits package.
Medicare’s Cost Challenge
The cost of Medicare has increased steadily since the program was established in 1965 and is projected to continue growing.
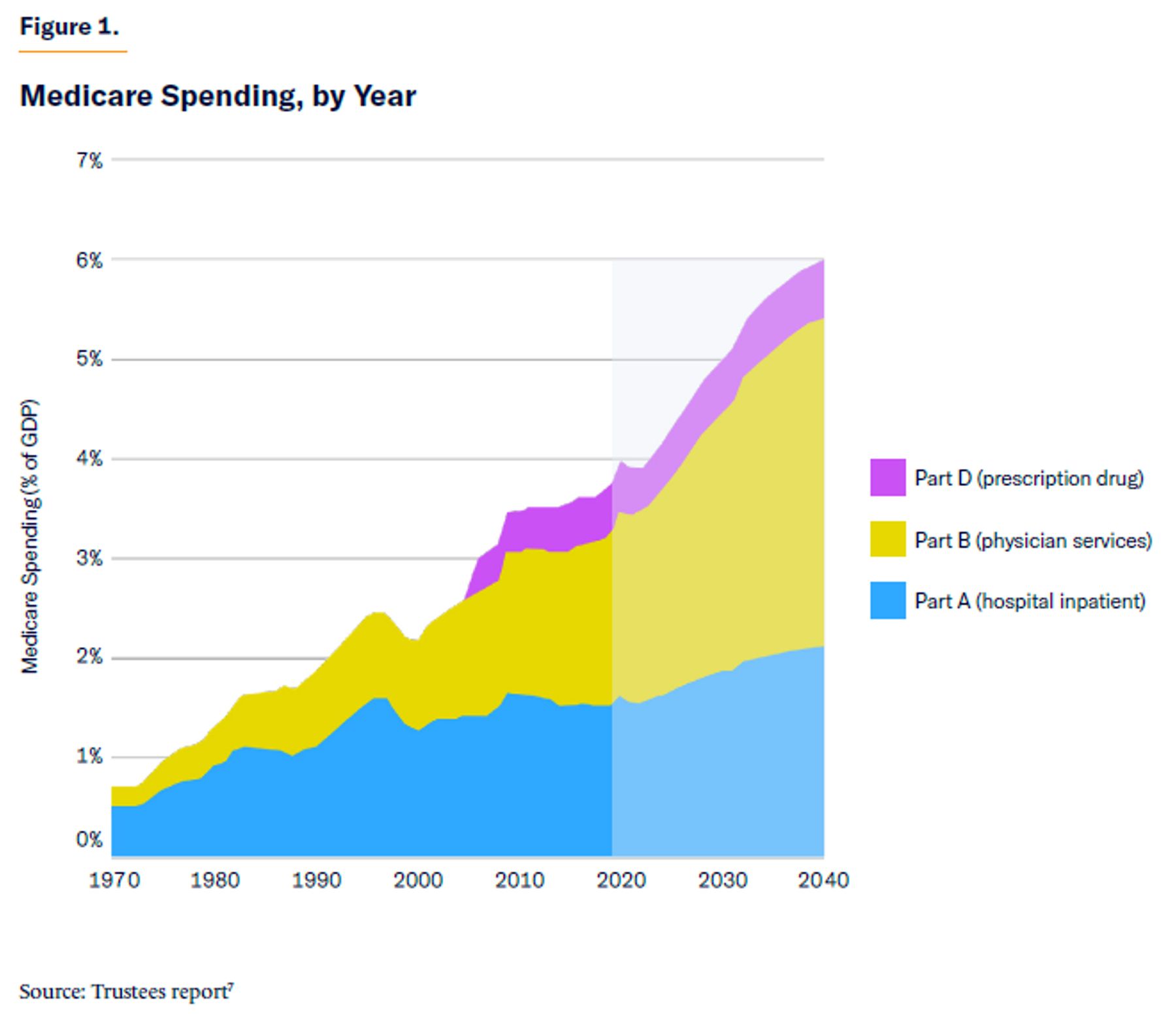
In 2020, federal spending on Medicare for the first time exceeded that on national defense.[1] The Congressional Budget Office (CBO) projects that in 2032, Medicare will spend $1.9 trillion—twice the level of expenditure on defense.[2] Medicare’s trustees note that the program’s cost has risen from 2.2% of GDP in 2000 to 3.9% in 2021, and they estimate that it will exceed 6.0% in 2040 (Figure 1).[3]
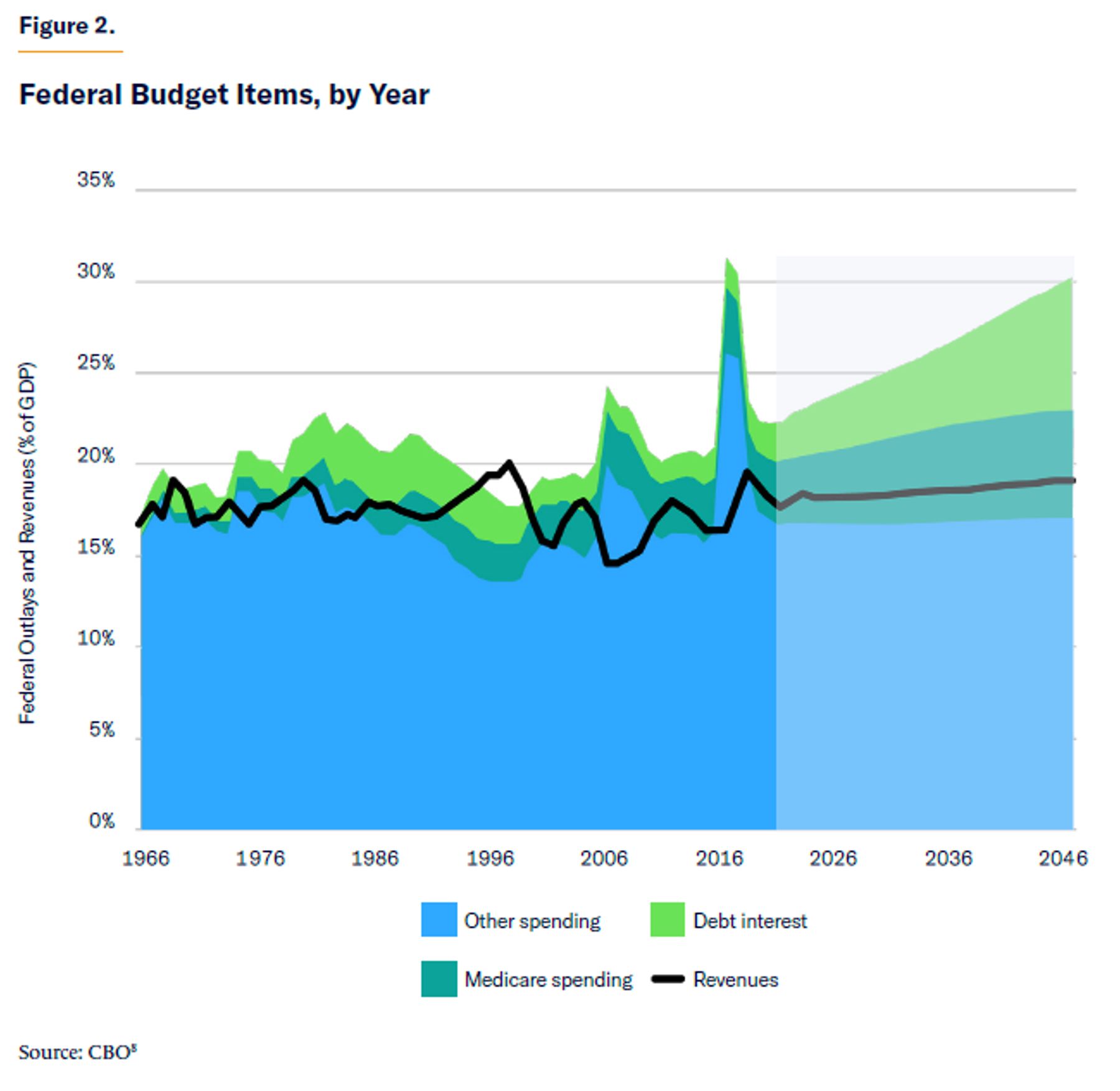
Such an increase in expenditure is unsustainable. According to CBO, the anticipated increase in Medicare spending will account for three-quarters of the 3.9% increase in the federal budget’s primary deficit (i.e., excluding interest payments) from 2022 to 2050.[4] Without reforms to Medicare, increases in tax rates, or cuts to other programs, interest payments on the federal debt will soar from 1.6% to 6.7% of GDP (Figure 2).[5] Beyond 2058, projected deficits “become so large and unsustainable that CBO’s model cannot calculate their effects.”[6]
Medicare’s Part A, which pays for inpatient hospital services, has traditionally been financed by a dedicated “Hospital Insurance” payroll tax. Medicare’s board of trustees anticipates that Part A expenditures will exceed the revenue from this tax in 2023 and that the program’s accumulated “trust fund” will be entirely depleted by 2028.[9]
The rising cost of Medicare not only burdens the federal budget but also seniors themselves. Medicare Parts B and D are partly financed by premiums paid by beneficiaries, which range from 25% to 85% of benefit costs, according to enrollees’ income levels. As Medicare costs increase, seniors and the disabled will face higher premiums.
To secure the support of hospitals and doctors for the launch of the Medicare program, Congress originally promised to pay medical providers according to the expenses that they incurred in delivering care to eligible beneficiaries. This caused the cost of hospital care to surge, as facilities were initially able to secure reimbursement for capital investments and expansions of capacity that they made. Spending on physician services was similarly pushed up by Medicare’s commitment to pay “customary, prevailing, and reasonable” charges, without greatly scrutinizing the value or appropriateness of particular reimbursement claims.[10]
Between 1967 and 1983, Medicare spending on hospitals soared from $3 billion to $37 billion, as hospitals competed by making enormous expenditures on cutting-edge technology, while facilities proliferated with little regard for efficient levels of equipment, staffing, and occupancy.[11] This fueled the rapid deployment of new medical technologies such as intensive care, renal dialysis, heart surgery, transplants, and diagnostic equipment.[12] In 1974, for example, there were only 20 CT scanners in the U.S.; by 1976, there were 400.[13]
As technology improved, more conditions could be diagnosed at an earlier stage—allowing a much greater number of interventions to effectively be pursued. From 1980 to 1995, the rate of cataract surgery among American Medicare beneficiaries increased more than fourfold.[14] Similar advances in orthopedic surgery led to an increase in total hip-replacement recipients, from 240,000 in 1980 to 2.5 million in 2010, while the number of knee-replacement recipients rose from 298,000 to 4.7 million.[15]
Ever since Medicare went into effect in 1966, policymakers have struggled to rein in the program’s cost. Within a few years, they began to limit annual increases in prices that providers could bill the program. In 1983, Congress fixed a schedule of payment amounts for hospitals treating inpatients with specific medical diagnoses, in order to limit the reimbursement that facilities could claim for them.[16]
The creation of fixed reimbursement rates gave hospitals a powerful incentive to cut their costs (typically by reducing the length of patient stays), which yielded the largest profits in their history.[17] The reform did slow the further compounding growth of hospital spending, from an average of 14% per year in 1965–82, to an average of 6% since then.[18]
Payments for services routinely provided in conjunction with a hospital stay (for physicians, anesthesiologists, follow-up care, etc.)—along with other outpatient procedures—were excluded from Medicare Part A’s diagnosis-related payments. Medicare Part B pays separately for each consultation, surgical procedure, drug, device, and diagnostic test that is employed, rather than providing fixed payments to treat patients with given diagnoses.
Separate fee schedules were subsequently established for physician and other services delivered on an outpatient basis under Medicare Part B. As fees for services are set in proportion to the cost of inputs, physicians have little incentive to minimize cost when determining a course of treatment. Thus, while the growth of inpatient hospital expenditures slowed during the 1980s, Medicare spending on Part B services picked up speed (see Figure 1 above).[19]
In 1992, Congress sought to rein in the volume of Part B services, by automatically reducing Medicare physician fees when the growth rate of service use per beneficiary exceeded that of the economy as a whole. But this mechanism squeezed clinicians’ real incomes without changing their individual incentives to increase service volumes, so fee cuts were repeatedly overridden by Congress, until the arrangement was eventually repealed in 2015.[21] While the growth of prices that Medicare pays for health-care services has been slowed, the increase in volumes has continued unabated.[22]
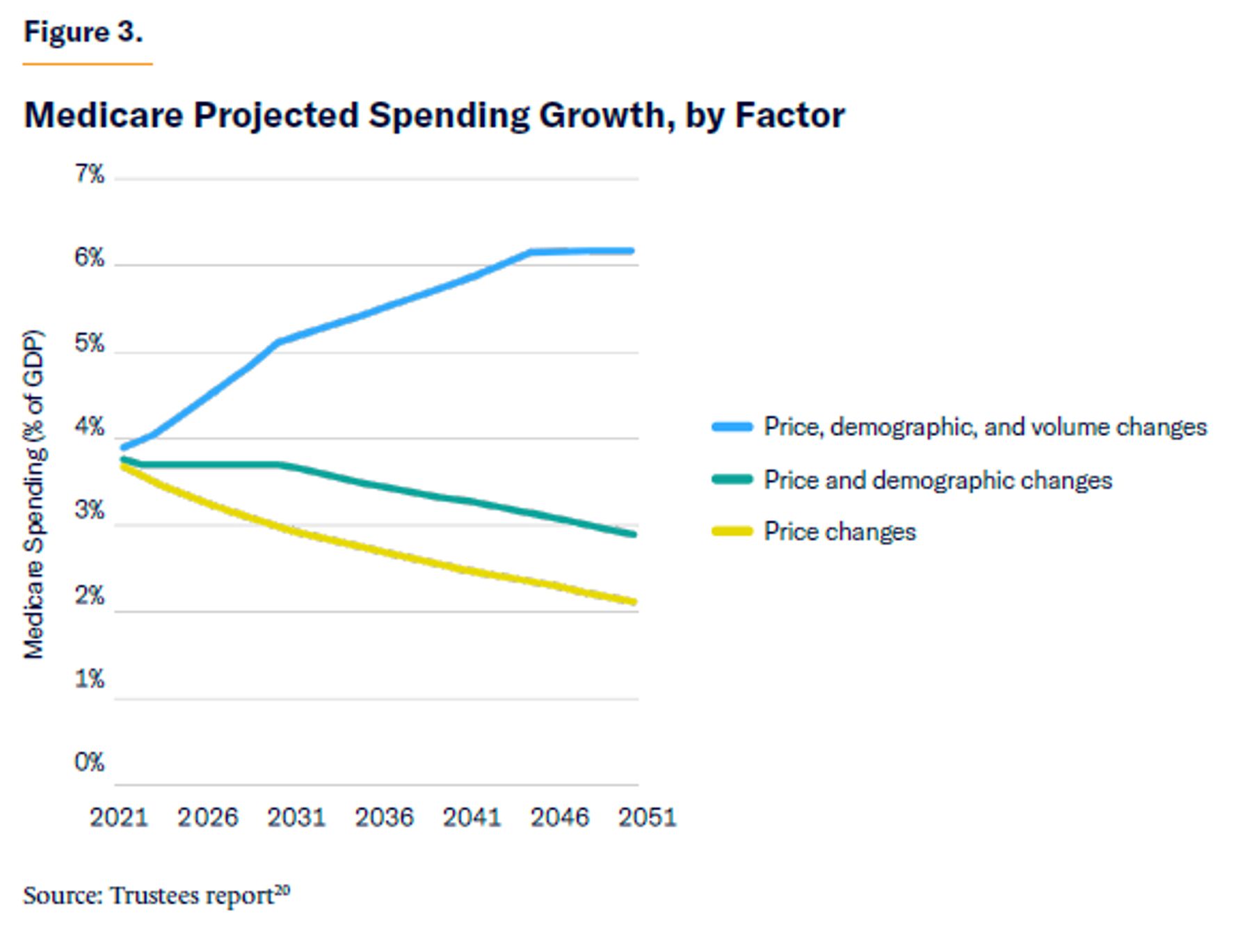
Under current law, Medicare’s trustees project that the prices that Medicare pays for medical care will increase at about the general level of inflation. They project a one-time surge in the program’s cost from 2000 to 2030, due to the retirement of the baby-boom generation, but they estimate that demographics will not substantially affect the program’s cost beyond that time. The bulk of the increase in the program’s future expenditure is expected to come from increases in the volume and intensity of service use.
The trustees’ estimates suggest that, given the prices that Medicare pays for existing medical procedures under current law, economic growth will be able to cover the costs associated with projected future changes to the age structure of the population.[23] But economic growth will likely be insufficient to cover the open-ended commitment to pay for whatever new medical procedures are developed and made available (Figure 3).[24]
Restraining New Service Costs
To keep the growth of Medicare costs at a sustainable level, it is therefore both necessary and sufficient to slow the addition of new services and volumes to the program. Fortunately, doing so is politically much less challenging than trying to deprive beneficiaries of services (and providers of revenues) that they are already accustomed to receiving.[25]
The increase in Medicare volumes is largely due to the establishment and increased utilization of new procedure codes. From 1997 to 2011, 85% of the increase in real per-capita Medicare spending was on newly created procedure codes.[26]
This trend appears to have continued. Table 1 shows the 10 procedures and services that accounted for the most fee-for-service spending under Medicare Part B in 2009. From 2009 to 2019, spending on these 10 procedures increased by only 13.9%, while Medicare Part B fee-for-service spending increased by 41.4%.[27] The price of these 10 procedures and services increased by an average of only 14.3%—less than the 19.2% general rate of inflation over the same period—while the volume of reimbursement claims for them declined by 0.4%, despite the number of enrollees in the basic Medicare Part B fee-for-service benefit increasing by 4.0% over that period.[28]
This remarkably modest increase in spending on existing codes cannot be fully explained by substitution away from the codes that were most popular in 2009 to a different set of codes that were popular in 2019. Total expenditure on the 200 highest-spending Level 1 (procedure) codes in 2019 was only 20.8% higher than it was on the top 200 codes in 2009.[29]
Table 1.
Highest Spending Part B Fee-for-Service Reimbursement Codes
| 2009–19, % Change in: | |||||
| CPT Code | 2009 Charges | Description | Spending | Volume | Price |
| 99214 | $6,534,736,194 | Office/outpatient visit (10–19 min.) | 70.2 | 47.5 | 15.4 |
| 99213 | $6,043,723,157 | Office/outpatient visit (20–29 min.) | 8.8 | –8.5 | 18.9 |
| 99232 | $3,313,715,475 | Subsequent hospital care | –0.9 | –9.7 | 9.7 |
| 66984 | $2,135,097,512 | Cataract surgery | 6.8 | 5.8 | 1.0 |
| 99233 | $1,987,644,579 | Subsequent hospital care | 30.6 | 19.2 | 9.6 |
| A0427 | $1,849,098,741 | Ambulance (emergency) | 15.7 | 6.4 | 8.7 |
| E1390 | $1,771,951,097 | Oxygen concentrator | –65.2 | –34.4 | –47 |
| 99285 | $1,433,482,586 | Emergency dept. visit | 39.4 | 36.4 | 2.2 |
| A0428 | $1,426,171,019 | Ambulance (nonemergency) | –29.2 | –26.7 | –3.4 |
| A4253 | $1,383,283,479 | Blood glucose test strips | –90.4 | –60.6 | –75.6 |
| Total | $27,878,903,839 | 13.9 | –0.4 | 14.3 | |
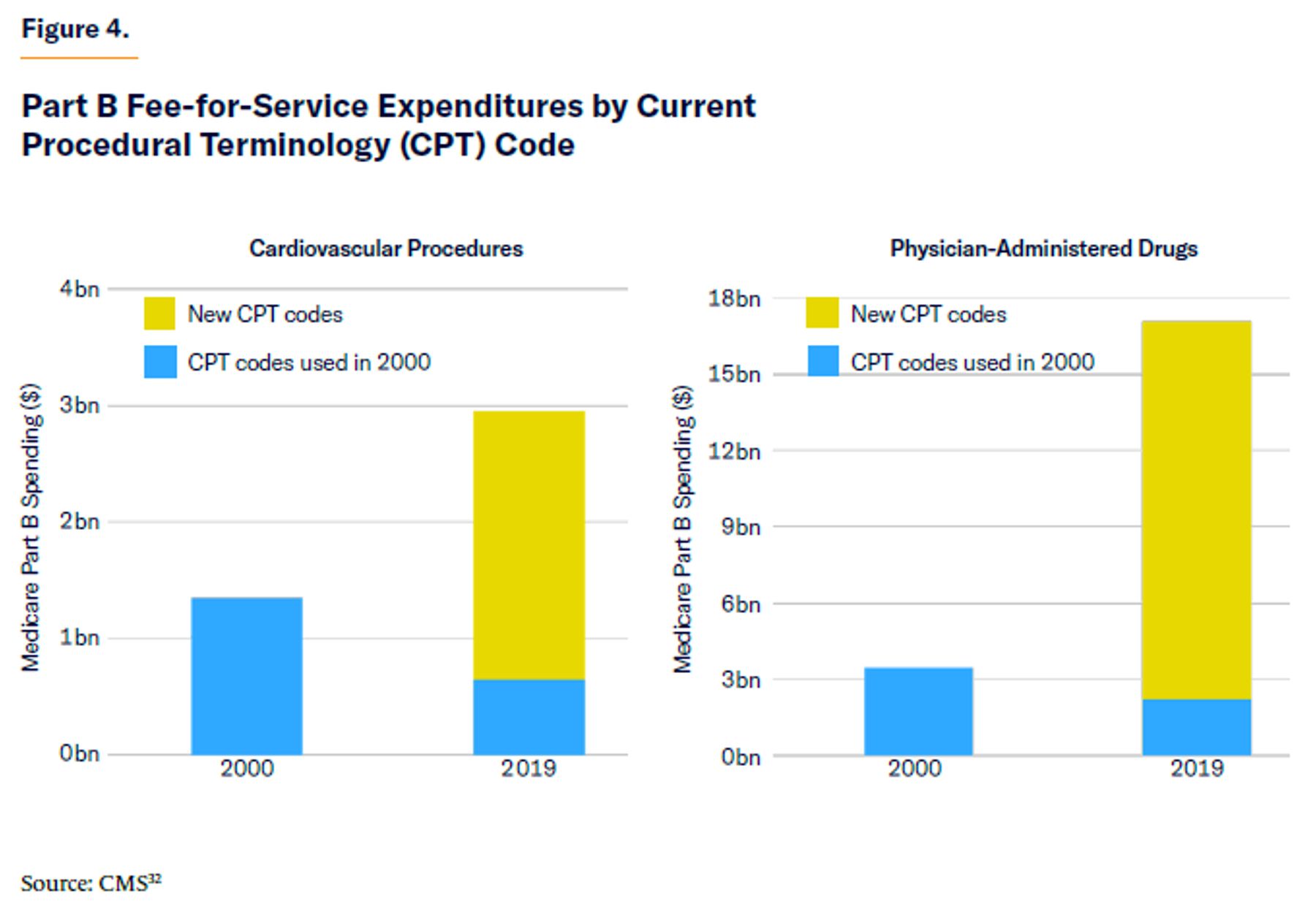
Recent increases in Medicare spending have been concentrated in medical specialties with the greatest proliferation of new billing codes. For instance, payments to physicians for cardiovascular procedures increased from $1.3 billion in 2000 to $3.0 billion in 2019—$2.3 billion of which was on service codes that did not exist in 2000. Similarly, spending on physician-administered drugs surged from $3.4 billion in 2000 to $17.1 billion in 2019—$14.9 billion of which was on codes that didn’t exist in 2000 (Figure 4).[31]
Whereas new drugs must demonstrate safety and efficacy in placebo-controlled trials to gain approval by the Federal Drug Administration, no such formal process is required for new surgical procedures. Whereas Medicare Part D prescription drug plans may require patients to try the most cost-effective therapeutics first, Part B generally pays for outpatient services (including physician-administered drugs) without regard to cost-effectiveness.[33]
Medicare Parts A and B are required to cover new products, services, and procedures deemed “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.”[34]
Medicare coverage for new services is typically expanded through “Local Coverage Determinations” (LCDs) by Medicare Administrative Contractors—private insurers that are responsible solely for processing claims and not for financing.[35] LCDs may restrict reimbursement to specific clinical settings, diagnostic conditions, or patient circumstances. However, because the contractors bear none of the additional expense, they have little incentive to rigorously enforce restrictions on reimbursements. Typically, they accommodate changes in practice styles and emulate new payments established by other payers. In rare cases, the Centers for Medicare & Medicaid Services (CMS) tries to harmonize conflicting LCDs through national coverage determinations—usually in an effort to ensure safe use, rather than to prevent needless expense—but these limits are also poorly enforced and have little effect on utilization or reimbursement.[36]
Some scholars have suggested that expansions of coverage to new products and procedures should be subject to regulatory cost-effectiveness assessments.[37] Over recent decades, presidential administrations of both parties have taken tentative steps to incorporate cost considerations into Medicare coverage policies. But these efforts have lacked a firm statutory basis, and officials have retreated in the face of pressure from beneficiaries concerned about being deprived of access to care, stoked by lobbying from medical providers that would lose revenues.[38] As a result, expansions of coverage are made almost entirely without considering—or even attempting to quantify—the additional costs to taxpayers.[39]
Fees for Medicare services are set by CMS through formal administrative rulemaking. For changes to the Part B fee schedule, CMS typically follows recommendations made by the American Medical Association’s RVS Update Committee (RUC). Federal law currently requires adjustments to fees for existing Part B physician services to be budget-neutral, but this requirement does not apply to the establishment of new payment codes for Part B services or to add-ons for Part A payments to hospitals for new technology.[40] In many cases, medical specialty societies seek to have new codes added precisely because they are exempt from budget-neutrality constraints.[41] From 1994 to 2009, 57% of changes to the physician fee schedule were due to the establishment of codes for new services, rather than budget-neutral adjustments to relative values.[42]
Over recent years, CMS regulatory changes have increased Medicaid’s annual expenditures by an average of 1.2% every year.[43] These annual increases in (unfunded) expenditures will have a compound effect; stopping them now would reduce the cost of Medicare from 4.1% to 4.0% of GDP in 2024, from 5.7% to 4.6% in 2040, and from 6.2% to 3.9% in 2060.[44]
Responsibility for adding new payment codes (which lies with CMS) is currently divorced from responsibility for paying for them (which ultimately rests with Congress). Attempts to restrain the incremental bureaucratic expansion of the program to cover new procedures, products, and services are likely to have little effect so long as they are considered in isolation from the additional cost that they impose.
As Mark Pauly correctly notes, “it is the technology-fueled and apparently inexorable growth of Medicare spending, not its possible current-period inefficiency, that makes Medicare as we know it infeasible in the relatively near future.”[45]
A Legislative Solution
Congressional approval and formal ratification should be required for the addition of new payment codes (under both Parts A and B) to take effect.
This would allow Congress to consider the cost-effectiveness of proposed incremental changes to the program, which will require it to find savings or additional revenues to pay for expansions of the standard benefits package that it deems worthwhile.
Every six months, CMS should submit any proposed additions to fee schedules (such as technology add-ons to prospective payments under Part A or new procedure codes under Part B), along with background information needed for the Medicare Payments Advisory Commission (MedPAC) and CBO to estimate costs in excess of the CBO baseline within a 10-year spending window. Both chambers of Congress should be required to consider the changes proposed by CMS, subject to debate time limits in the U.S. Senate (i.e., exempt from the filibuster), so long as the proposed package of changes (including pay-fors) is estimated to be budget-neutral by MedPAC/CBO.
The Role of Medicare Advantage
Medicare Advantage (MA) can do much to reduce expenditure on low-value procedures, while promoting the interests of Medicare beneficiaries and taxpayers alike.[46] But the expansion of MA alone will not remedy inappropriate cost increases resulting from expansions of the standard benefits package because MA plans are required to pay for all standard services. Furthermore, any increase in the cost of the traditional Medicare benefit, resulting from the addition of procedures to the basic benefit, will push up benchmark payments and costs to taxpayers.
Under the legislative reform proposed here, however, MA plans would remain able to cover new services, devices, and procedures—even those that Congress has not approved—without adding costs to federal taxpayers. In many cases, this would successfully relieve political pressure to expand public spending on the basic benefits package.
For new cost-reducing technologies, this would be entirely straightforward, as MA plans have the authority and incentive to pay for them out of existing revenues. For technologies that improve quality but also increase costs, plans could either: (1) use savings generated in the delivery of the standard Medicare benefit; or (2) charge an additional premium for access to costlier newly developed services.[47]
Some have argued that Medicare Advantage plans would be averse to expanding coverage of costly technology because doing so could lead to an influx of unprofitable beneficiaries with relatively high expected treatment costs.[48] But this dynamic is mitigated by risk-adjustment payments, which compensate plans for attracting relatively costlier enrollees.[49] Indeed, the normal incentives for MA plans—to add services that reduce overall patient costs (e.g., by preventing expensive hospitalizations) or to increase revenues (by keeping patients alive)—are even stronger when it comes to higher-risk patients. The incentives to add new technologies are, however, contingent on their cost-effectiveness.
In practice, private insurers have been remarkably quick to expand coverage to newly developed technology.[50] In general, private payers provide broader access to newly developed medical devices than Medicare does about a quarter of the time, and they provide more restrictive access about a quarter of the time.[51] MA plans already offer enhanced access to services that are disproportionately attractive to those with high-cost chronic conditions. For instance, MA patients with end-stage kidney disease who received additional disease management services had significantly lower rates of hospitalization and mortality than matched patients who received only the basic Medicare benefit.[52] Similar improvements have been noted for diabetes patients.[53]
Nonetheless, risk adjustment does not completely eliminate the incentive for plans to avoid higher-cost enrollees.[54] It will therefore remain necessary to continue to add demonstrably highly effective new procedures to the basic Medicare benefits package to ensure that they are not omitted by MA plans.
Implications for Reform—Medical Investment
It may reasonably be feared that investors will be hesitant to invest in the development of new medical technology if congressional approval were required before such technologies could be covered by Medicare. But providers would retain the ability to lobby aggressively for the expansion of coverage to newly developed services, and they will be able to draw on millions of Medicare beneficiaries as allies in that endeavor.
However, this may not be sufficient to assure investors in new therapies, for which development costs prior to approval are enormous but production costs are typically minimal—such as with high-priced cancer drugs. In such a circumstance, members of Congress might be tempted to obstruct approval in order to insist on lower prices, which would make uncertain investments much less attractive ex ante.[55]
But this tactic is unlikely to prove effective. Statutory pricing formulas would not be changed by merely requiring Congress to ratify expansions of coverage. Indeed, whatever immediate budgetary savings may accrue from altering that reimbursement formula would be dwarfed by the chilling effect on other investment decisions.[56] In other words, drug investors would remain protected by the same political dynamic that currently protects their investments. In fact, establishing a clearer separation between coverage decisions and pricing policy would likely relieve political pressure to bend the latter in order to generate ad hoc reductions in expenditure.
Medicare is likely to be confronted with a growing array of high-cost coverage decisions in coming years. The expansion of coverage to drugs like Aduhelm, a new Alzheimer’s medication with enormous costs and debatable effectiveness, will necessarily lead policymakers to weigh the additional expense to taxpayers against the additional value to Medicare beneficiaries. Such determinations can rightly be informed by stakeholders, scholars, and administrators. But the ultimate responsibility for making these decisions appropriately rests with Congress, as it is the institution responsible and accountable for both sides of the ledger.
Conclusion
Medicare’s steadily increasing burden on the federal budget is largely the result of the program’s commitment to pay for ever-increasing volumes of new medical products, procedures, and services—most of which are currently approved without scrutiny of their cost-effectiveness.
Congress should be required to approve additions to Medicare fee schedules before they take effect. This would preserve existing benefits for all beneficiaries without increasing costs to taxpayers, and it would ensure that incremental expansions of the program’s standard benefits package will be subject to debate about whether they are worth the expense and how they will be paid for.
About the Author
Chris Pope is a senior fellow at the Manhattan Institute. Previously, he was director of policy research at West Health, a nonprofit medical research organization; health-policy fellow at the U.S. House Committee on Energy and Commerce; and research manager at the American Enterprise Institute. Pope’s research focuses on health-care payment policy, and he has recently published reports on hospital-market regulation, entitlement design, and insurance-market reform. His work has appeared in, among others, the Wall Street Journal, HealthAffairs, U.S. News & World Report, and Politico.
Pope holds a BSc in government and economics from the London School of Economics and an MA and PhD in political science from Washington University in St. Louis.
Endnotes
Photo by Kameleon007/iStock
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).