How to Reform Correctional Mental Health Care

Photo: Hans Neleman/Stone via Getty Images
Executive Summary
“Trans-institutionalization” refers to the shift of seriously mentally ill adults from the care of psychiatric institutions to correctional institutions. Beginning in the 1950s, public mental health agencies have pursued the deinstitutionalization of the seriously mentally ill. These government agencies intended to meet that goal through creating a system of community-based care to replace the asylum-based systems. Deinstitutionalization did not succeed as planned. Consequently, jails and prisons became the custodians of hundreds of thousands of seriously mentally ill adults who in previous eras would have been committed to an asylum.
Some dispute the magnitude of trans-institutionalization. But no one denies the high rate of serious mental illness among the incarcerated, or that jails and prisons are poor settings in which to treat serious mental illness. Correctional mental health care now stands as one of the most important mental health care systems in the nation. Jails and prisons are legally obligated to serve the seriously mentally ill, whereas community-based systems are not. More effective community-based mental health remains an important goal to pursue. But equally important is the reform of corrections-based systems. Better correctional mental health care systems will benefit both community systems and the seriously mentally ill themselves.
This report will explain how corrections-based systems function. It will place those systems in the context of debates around “jail abolition,” explain their workforce and financial challenges, and recommend the following reforms:
- State governments should assume more responsibility for funding jail-based mental health care.
- Correctional mental health systems have special responsibility to the seriously mentally ill and are justified in targeting resources accordingly.
- Collect, keep, and report better data.
- Repeal Medicaid’s Institution for Mental Diseases (IMD) exclusion.
- Correctional institutions should make more use of long-acting injectables during discharge.
- Eliminate overuse of administrative segregation (solitary confinement); do not abolish it.
- Do not use telehealth when reliance on onsite clinical staff is feasible.
The Problem
Magnitude
Seriously mentally ill Americans are incarcerated at a rate disproportionate to their share of the general population. The federal government estimates that 6% of American adults are seriously mentally ill.[1] The rate of serious mental illness in jails and prisons, though uncertain (Appendix 1), is likely three to four times that rate. Table 1 applies conventional estimates of that rate to current jail and prison inmate counts, projecting about 300,000 seriously mentally ill incarcerated Americans.
Table 1
Estimated Number of Seriously Mentally Ill (SMI) Adults in U.S. Jails and Prisons, 2022
| Rate of SMI | Total Pop. | Est. # SMI | |
| Jails | 20% | 663,100 | 132,620 |
| Prisons | 15% | 1,230,100 | 184,515 |
| Total | 317,135 |
Source: “Serious Mental Illness (SMI) Prevalence in Jails and Prisons,” Treatment Advocacy Center, September 2016; E. Ann Carson and Rich Kluckow, “Prisoners in 2022—Statistical Tables,” U.S. Dept. of Justice, Office of Justice Programs, Bureau of Justice Statistics, November 2023; Zhen Zeng, “Jail Inmates in 2022—Statistical Tables,” U.S. Dept. of Justice, Office of Justice Programs, Bureau of Justice Statistics, December 2023. See also Jennifer Bronson and Marcus Berzofsky, “Indicators of Mental Health Problems Reported by Prisoners and Jail Inmates, 2011–12,” U.S. Dept. of Justice, Bureau of Justice Statistics, June 2017. For a discussion of why the rate may be higher in jails than prisons, see Emily D. Gottfried and Sheresa C. Christopher, “Mental Disorders Among Criminal Offenders: A Review of the Literature,” Journal of Correctional Health Care 23, no. 3 (2017): 336–46.
Seriously mentally adults in correctional settings outnumber the homeless and those in mental health treatment facilities (Figure 1).
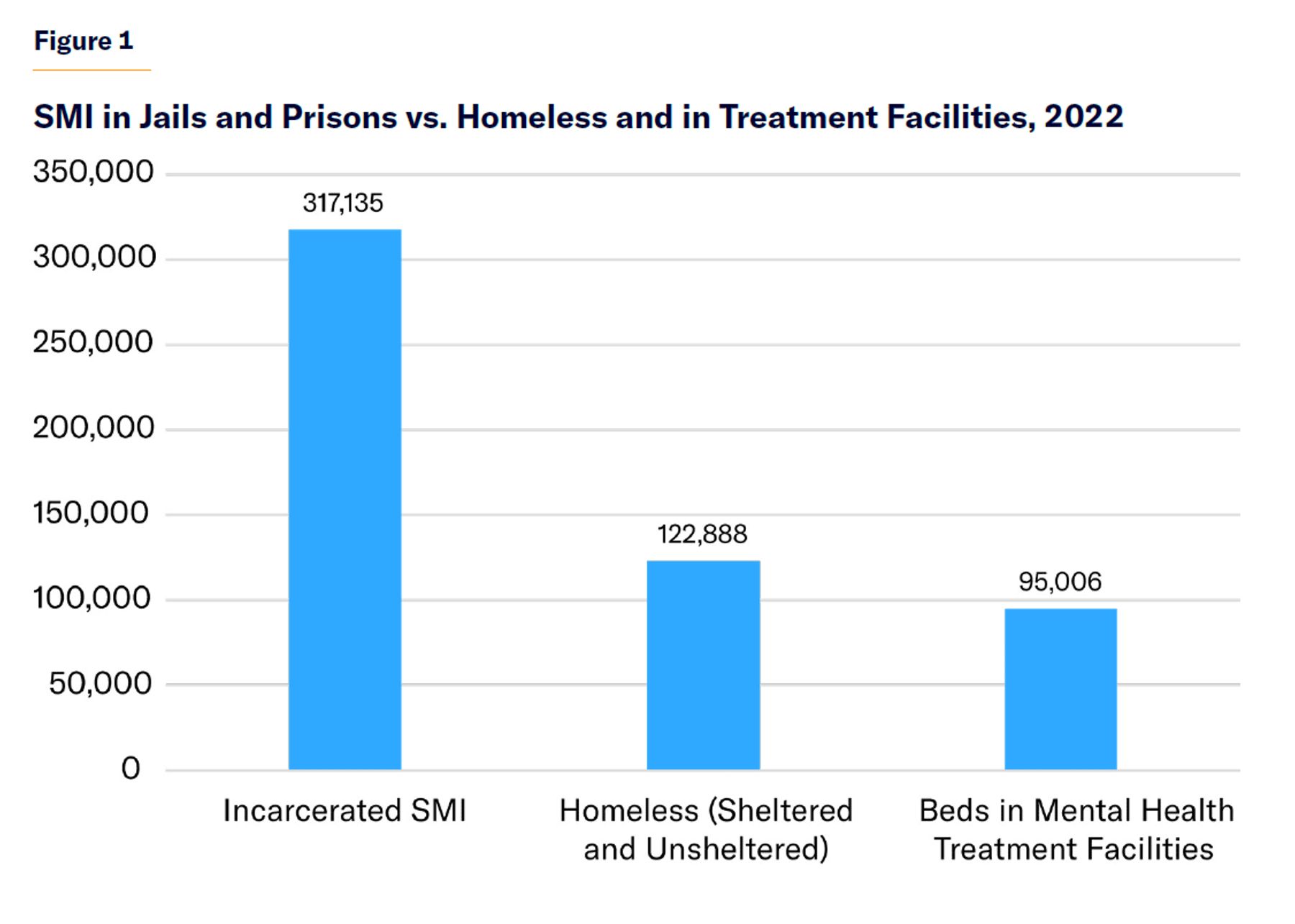
Of the two-thirds of seriously mentally ill adults who received treatment in the past year, about 4%, or 390,000, received treatment in a correctional setting, according to federal data.[2]
The high rate of serious mental illness in correctional settings poses two policy challenges. First, virtually every incarcerated-related adverse outcome for inmates in general is worse for the seriously mentally ill: victimization,[3] rape,[4] suicide,[5] administrative segregation,[6] recidivism.[7] They are more likely to fail in community supervision (probation and parole).[8] Upon discharge, mentally ill inmates have less money in their prison canteen accounts because they participate in work programs at lower rates and are more isolated from their families.[9] They are thrown “welcome home” parties less frequently than ex-offenders who are not mentally ill and are more likely to be unemployed after release.[10]
Second, seriously mentally ill offenders stand at the intersection of policies with conflicting priorities. The goal of mental health policy is to reduce the rate of untreated serious mental illness. Because of the priority that jails and prisons place on security, and the character of the inmate population, seriously mentally ill offenders lack meaningful daily activities, are in fear-inducing environments, lack access to positive relationships, and lack privacy. Their lives have an artificial structure utterly dissimilar to life in the community. All those factors diminish the likelihood of successful treatment. Federal agencies estimate that the rate of nontreatment for mental health among jail and prison inmates is about two-thirds, whereas that rate is only one-third for the population as a whole.[11]
Causes
Trans-institutionalization is the most common explanation for the concentration of seriously mentally ill people in jails and prisons. The supposition is that many of the seriously mentally ill in U.S. jails and prisons are people who would have been committed to state asylums decades ago; and that—had deinstitutionalization not happened, or been executed more competently—the rate of serious mental illness would now be lower in jails and prisons.[12] This thesis has its origins in an old theory that, in any given society, a certain portion of individuals are so troubled that they must be confined either to a correctional or psychiatric institution.[13] The standard criterion for involuntary psychiatric commitment is dangerousness caused by a psychiatric disorder. The hundreds of thousands of seriously mentally ill adults in jails and prisons are, often enough, dangerous and also have psychiatric disorders. Their confinement to jails and prisons instead of psychiatric hospitals thus seems to represent a “category error” caused by the failings of deinstitutionalization.
The trans-institutionalization thesis is difficult to prove because of uncertainty over prevalence rates of serious mental illness in jails and prisons, both now and in the past (Appendix 1). Progressive critics of trans-institutionalization prefer to see the high numbers of seriously mentally ill in jails and prisons as a side effect of “mass incarceration.” Deinstitutionalization and “mass incarceration” are two large-scale social changes that took place simultaneously. Therefore, the effects of each movement are hard to disentangle. Between 1970 and the present, the number of public psychiatric hospital beds declined by about 340,000, and the number of people in jails and prisons rose by about 420,000 and 1.1 million, respectively.[14] Progressive critics believe that there are more seriously mentally ill people in jails and prisons because there are more people in jails and prisons; they doubt that the rate of serious mental illness among the incarcerated has changed over the decades.[15]
This dispute has policy consequences because if hundreds of thousands of seriously mentally ill became incarcerated because government cut too many psychiatric hospital beds, investing more in beds is the logical solution. If it happened because of “mass incarceration,” the logical solution would be to scale back the use of jails and prisons.
Certainly, the notion that the institutionalized population circa the 1950s was transferred, en masse, to jails and prisons, merits qualification. As shown in Table 1, the number of seriously mentally ill adults in jails and prisons is more than 300,000. The institutionalized population in the 1950s, adjusted for population, would be more than a million. Some groups who left psychiatric hospitals during deinstitutionalization were not transferred to jails and prisons—for example, seniors with dementia.[16] Many asylum patients were not dangerous but simply considered “in need of treatment,” the legal standard for civil commitment (parens patriae) that the “dangerousness” standard replaced via civil rights reforms in the 1970s.[17] Other settings in which seriously mentally ill adults are now found in greater numbers than they were in the asylum era include: (1) living with their families; (2) in homeless shelters; and (3) living on the streets.[18] Many live highly unstable lives, but, even then, they might not have been “trans-institutionalized” so much as they are riding an “institutional circuit.”[19] Trans-institutionalization seems to imply that one form of long-term confinement, in an asylum, was historically exchanged for another long-term confinement, in a correctional facility.
Even if the seriously mentally ill have not been transferred from asylums to correctional facilities on a one-to-one basis, trans-institutionalization likely accounts for a significant portion of the problem,[20] for five reasons:
- Historical evidence attests that not only were jails[21] used to confine the mentally ill before state asylums were built; mentally ill inmates were directly transferred from jails to newly built asylums in the mid-nineteenth century.[22] By the post–Civil War period, the rate of serious mental illness in correctional settings was very low.[23]
- While the rate of serious mental illness in jails and prisons before deinstitutionalization was never zero,[24] the “criminalization of mental illness” has not been a consistent subject of public concern throughout U.S. history. Concerns over too many mentally ill in jails ran high in the early nineteenth century and have run high since the 1980s. They did not run nearly as high throughout the asylums’ long expansion period.[25] Certainly, jails and prisons in previous eras gave far less consideration to seriously mentally ill inmates than do contemporary correctional architects and design consultants. The prevalence rate was likely lower then than now.[26]
- Many employees of criminal justice and mental health agencies whose careers overlapped with the decline in state hospital beds and rise in incarcerated mentally ill offenders strongly believed that they witnessed trans-institutionalization in real time.[27]
- Even if prison sentences for crack cocaine, for instance, weren’t common in the 1950s, short jail stays for public drunkenness were. That’s a problem for those who suggest that “increased criminalization of disturbed and disturbing behavior”[28] explains the phenomenon. True, many seriously mentally ill are incarcerated on low-level charges, especially for drugs.[29] But it’s also true that police departments have always been involved in addressing public disorder.[30]
- The community-based system that deinstitutionalization proposed was supposed not only to differ from the asylum-based system but to be superior to it. “Community integration,” still the goal of public mental health authorities, should mean that the seriously mentally ill offend at rates close to the rates at which ordinary Americans offend. That hundreds of thousands of seriously mentally ill Americans are incarcerated is therefore, on its face, evidence of the failings of the community system that deinstitutionalization created.
Trans-institutionalization is especially clear in the case of rural communities. In counties where there is practically no community mental health system and where psychiatric hospital-based care is less accessible than was the case in the 1950s, the seriously mentally ill sometimes have better access to care in a county jail than through any other program.[31] In large urban areas, community health systems are more robust, but so are urban correctional health systems. Thus, there is still the possibility that, in big cities, access to certain health services will be superior on the inside than the outside for mentally ill offenders.[32] Big-city police departments sometimes report using “mercy bookings” or “compassionate arrests” for the difficult cases for which community mental health programs cannot or will not take responsibility.[33]
The System
Operations
Seriously mentally ill adults can become “criminal justice–involved” in multiple ways. In recent years, special interventions—such as crisis response training for police, as well as mental health courts—have been designed with the mentally ill in mind. The goal of these programs is to divert the seriously mentally ill from deeper involvement in the criminal justice system. Those for whom diversion fails wind up in jails and prisons.
Correctional mental health services are delivered at the beginning, middle, and end of the incarceration process (Table 2).[34]
Table 2
Correctional Mental Health Care, by Phase
| Booking/Intake | Evaluation of whether charged inmates are competent to face their charges Diagnosis, including for substance abuse Classification for dangerousness and eligibility for special housing |
| Confinement | Dispensing medication and evaluating the need for changes in medication Providing psychosocial interventions such as dialectical behavioral therapy Remediating behavior-related problems with correctional staff Advocacy on behalf of inmates |
| Discharge | Establishing connections with community-based programs |
Many correctional systems have recently expanded mental health services.[35] They have sometimes been legally required to do so. At the same time—much as the expansion of school-based mental health services has been justified as a way to better meet schools’ educational goals—there has been a growing belief that mental health programming can contribute to better-functioning jails and prisons. Mental health professionals specialize in treatment, and if treatment can make inmate populations less dangerous and more compliant with rules, corrections staff often welcome more spending on mental health in jails and prisons. Correctional professionals, though typically seen as political conservatives, sometimes take positions with the medical community and against fiscally conservative politicians, such as on expanding Medicaid both inside and outside jails and prisons.[36] Mental health staff can help determine whether malingering (feigning an illness to seek advantage) is real or not and whether a psychiatric symptom stems from substance abuse or from an underlying mental illness. They can also provide assistance in regulating the use of administrative segregation (when a prisoner is housed separately, or solitary confinement) and assess whether rules infractions stem from lack of treatment, and therefore might be better addressed through treatment than with punishment.
Jails v. Prisons
Most prisons are run by state governments and hold sentenced inmates for terms of confinement that exceed one year. Jails are generally run by counties and mostly hold inmates on a pretrial basis and for short-term sentences. Both are host to large numbers of seriously mentally ill inmates (as displayed in Table 1). Jail-based mental health differs from prison-based mental health. Because lengths of stay in jails are shorter and more unpredictable, that makes it more difficult for mental health staff to design and implement an effective treatment regimen and plan for discharge. Inmates, when sent to prison, are, on average, stabler than when entering jails, as they have already been assessed and likely have received at least some treatment. Inmates arrive in jail directly from the streets and at all hours.[37] By contrast, prison inmates arrive on a more regular schedule. These factors, among others, make intake assessments a more complicated proposition for jails than for prisons.
Reforming jail-based mental health services is more urgent than reforming prison-based mental health services because the magnitude of the problem is greater (far more people experience incarceration in jail than prison),[38] and the rate of serious mental illness runs higher and outcomes are worse. The suicide rate in jails is about twice that of the rate in prisons.[39] But reforming jail-based programs is harder because short stays are less conducive to proper treatment and medical economies of scale are much easier to realize in prisons, which run much larger than in jails.[40]
Jails are to prisons as emergency rooms are to hospitals.[41] The“churn” among the inmate population creates poor conditions for any kind of mental health intervention, from deep-dive talk-therapy examinations of past traumas to extended trial-and-error efforts to settle on the right medication regimen. The receipt of therapy is estimated to be twice as high in prisons (26%) than jails (13%).[42] The prison environment is more conducive to effective but complicated-to-administer medication interventions such as clozapine.[43] (In general, it’s easier for clinicians to discern whether people are taking their medications in a correctional setting than in the community.)[44]
Jail- and prison-based mental health services are provided by clinical personnel employed directly by state or local government, or a private contractor.[45] Governments invoke various rationales to justify why a private or government-run system of correctional health is superior. One advantage of using a private vendor may be superior cost management. Advantages of using government health employees may include better data-sharing and other modes of coordination between corrections systems and other public agencies.[46] However, either arrangement can be run competently or poorly.
Funding
Funding comes directly out of government budgets. Because of the federal Inmate Exclusion Policy, Medicaid cannot be used to pay for correctional health care, nor will Medicare (relevant, in this context, to inmates with disabilities, including psychiatric disabilities) pay.
Trans-institutionalization has caused a significant fiscal shift from states to localities. State governments funded the old asylum programs. Unburdening themselves of those programs’ often-considerable costs was one major motivation for why states pursued deinstitutionalization. Much of the cost of mental health care for non-incarcerated seriously mentally ill individuals who, in a previous era, would have been confined to a state asylum is now borne by Medicaid (a joint state-federal program). For the incarcerated, that cost is borne by whatever government manages the correctional institution that they are confined to, meaning counties, in the case of jails. Fiscally, state governments were a major “winner” in trans-institutionalization and county governments were major losers.
Administration
Trans-institutionalization has resulted in a much more fragmented and inefficient system of care. Most jails in America are very small,[47] though all are required to provide both mental and mainstream health care. The old asylum programs were massive, confining hundreds, and often thousands, of seriously mentally ill adults on one campus. Many jails are too small to provide truly dedicated “corrections-based” mental health programming.
Recruitment is a chronic and pervasive problem in correctional medicine.[48] Aside from, obviously, fears associated with working in a locked environment inhabited by criminals,[49] clinical staff might also avoid working in corrections because of the risk of lawsuits,[50] having to work with patients who, aside from the acuity of their psychiatric problems, have committed violent and sexual offenses against women and children[51] and who exhibit extraordinarily disturbing and predatory behavior less often encountered in community programs.[52] Rural communities have a shortage, often even a total absence, of mental health professionals.[53] Jails in such communities may provide mental health services by a part-time nurse with minimal background in mental health and certainly no specialized training in working with the seriously mentally ill. Urban systems face competition from community programs with more attractive pay and working conditions. In coming years, the mental health field is expected to experience a shortage of psychiatrists, the occupation most closely associated with serving the seriously mentally ill, and demand from individuals with nonserious mental disorders is expected to increase.[54] Two results of ongoing personnel shortages in correctional mental health care are that the use of telehealth is certain to continue to grow, and the fiscal strains of correctional mental health should be expected to grow as well.
The work is not without attractions, though. Seriously mentally ill inmates lack easy access to illegal drugs, which are a major barrier to successful treatment. Prisons, at least, offer the ability to work long-term with patients, in contrast to the more erratic modes of caring for the seriously mentally ill frequently found in community-based and even hospital-based settings. And, because third-party reimbursement is not a factor, clinicians are spared the administrative hassles associated with dealing with insurance companies and are thus able to focus more exclusively on delivering care.
Legal Considerations
In the community, seriously mentally ill adults have no right to mental health care and the system has no obligation to provide them with treatment. In correctional settings, however, incarcerated Americans may be said to have a “right” to mental health care in two respects. The first is through competency restoration. Americans cannot face criminal charges if they are so mentally unfit as not to understand the adjudication process. The process of making offenders mentally fit to stand trial, so that they may “aid and assist” in their own defense, is known as competency restoration. This process often involves basic instruction about courts and law and psychiatric treatment.
Second, even for inmates who are competent to stand trial but still seriously mentally ill, courts have located a right to mental health care in the Eighth Amendment’s prohibition of “cruel and unusual punishments.”[55] Courts reasoned that placing an obligation on correctional systems to provide health care is only fair, given that inmates can’t realistically operate as free health-care consumers.[56] Estelle v. Gamble speaks of a right to health care when systems, as a result of “deliberate indifference,” neglect inmates’“serious medical needs.”[57] Legal experts therefore advise correctional systems that they are not formally obligated to provide care for milder mental disorders or substance abuse disorders,[58] though many systems do provide those services.
There is no special obligation for anyone incarcerated to accept treatment. Involuntary psychiatric treatment is sometimes pursued for jail and prison inmates,[59] but the legal standards are no different from those for seriously mentally ill individuals not involved with the criminal justice system. The 1980 Supreme Court ruling in Vitek v. Jones[60] prohibited governments from transferring seriously mentally ill inmates from correctional facilities to psychiatric hospitals on simply a need-for-treatment basis.[61]
The legal system has been highly involved in the expansion of correctional mental health care in recent decades. One 2023 analysis found about 50 examples of consent decrees having to do with mental health conditions in prisons since 1972.[62] The federal Department of Justice has made mental health conditions a focus of many of its “pattern or practice” lawsuits, in which the department attempts to establish that discriminatory actions were the defendant’s regular practice, rather than isolated instances. Correctional professionals’ conferences and trade publications devote extensive attention to preparing for and responding to lawsuits. The threat of litigation has motivated the push to develop and implement accreditation standards for health care in jails and prisons. Many embrace the view that litigation has had a positive development for seriously mentally ill inmates.[63] The Cook County jail, led by Sheriff Tom Dart, would be an example where dutiful compliance with a court order led to the eventual lifting of that court order and a general improvement in that correctional system’s reputation.[64]
Judges and lawyers can sometimes empower stakeholders within correctional systems who support increased spending and better services but lack sufficient political support to effect those reforms on their own.
But litigation is not always successful. The Fulton County Jail in Georgia, in contrast to that of Cook County, would be an example where successful compliance with a court order is not seen as having led to a permanent and complete improvement in the jail’s conditions.[65] In New York City, a 2003 settlement established comprehensive discharge planning services for all mentally disordered inmates leaving the city jails.[66] But untreated serious mental illness is still considered a crisis in NYC, and the connection with homelessness particularly close. Also, Los Angeles County has not complied with the terms of a 2015 court order, partly because that would require building a new jail, an idea that local progressives, who supported the original settlement, currently oppose. The threat of litigation makes some correctional leadership and staff feel that they are considered guilty until proven innocent and thus makes them defensive and wary of transparency.
Some systems have developed well-regarded programs unprompted by outside legal pressure. Examples include Lane County, Oregon, and Franklin County, Ohio.[67] Lane County operates a wellness program for seriously mentally ill inmates that was developed at the initiative of correctional staff. Franklin County recently built a new jail, the plans for which gave extensive design consideration to the needs of seriously mentally ill inmates.
Jail Abolition
That large numbers of seriously mentally ill adults are incarcerated is a problem that has been recognized for decades.[68] However, discussion of solutions has taken on a new character, in how it intersects with the broader decarceration debate. Years ago, mentally ill offenders were thought of as having a “double stigma” that made them uniquely suitable for confinement and uniquely poorly suited for community-based alternatives to incarceration.[69] More recently, criminal justice reformers, especially those associated with the “abolition” movement, have argued the opposite: mentally ill offenders are less appropriate for confinement, and more suitable for community alternatives, than offenders without mental illnesses. Decarceration strategists often frame the high rate of serious mental illness among the incarcerated as creating an opportunity for large-scale jail and prison reductions.[70] This “new insanity defense,” which holds that special leniency is owed to incarcerated Americans with a mental disorder, helps the modern criminal justice reform movement establish itself on practical and scientific principles. It is progressives’ version of the category error: mentally ill offenders are “mad, not bad.”
The degree to which correctional programs can rehabilitate any offenders has long been a disputed issue. Conservatives were once closely associated with the idea that “nothing works”;[71] but more recently, that attitude has been more closely associated with progressives involved in the abolitionist movement. In Los Angeles County and Massachusetts,[72] abolitionists have prevented governments from replacing old facilities (Men’s Central Jail and MCI-Framingham); and in New York City, they persuaded policymakers to adopt the “Close Rikers” jail reduction plan that proposes unreasonably low bed-capacity targets.[73]
Advocates decry arrests of seriously mentally ill individuals for “nonviolent, minor offenses” such as “shoplifting and petty theft.”[74] But not only do the “violent” and “nonviolent” offender categories parse more cleanly in theory than in practice;[75] offenders facing less serious charges who have serious behavioral programs are some of the hardest to serve effectively through diversion and community-based programs.[76] And, viewed outside the mental health context, policymakers and the broader public do not view theft as a “minor” problem.
One city in which that is so is Portland, Oregon. Multnomah County (of which Portland is the county seat) has scaled back its use of incarceration as a result of progressive prosecution policies and increased interest in “innovative pre-trial diversion services.”[77] In the year before Covid, the monthly average daily population in Multnomah County jail hovered at about 1,110, compared with about 860 over the most recent 12 months.[78] But during the same span, average monthly reported property crimes rose from 4,000 to 4,500. It is not obvious that the local retail-theft wave can be checked without increased use of jail.
Government diversion efforts are eventually fated to reach a point of diminishing returns, and the need to rehabilitate offenders must be balanced against risks to the community. Community programs—the favored solution of abolitionists—benefit from well-run correctional programs. These programs take responsibility for cases too dangerous to be handled by community programs; and they stabilize seriously mentally ill individuals between intake and discharge. Investing in community and correctional mental health programs is thus not an either/or.
Many jails and prisons are decades old and in need of replacement because of public infrastructure management and because they were not designed to accommodate the care and treatment of the seriously mentally ill. They were designed for a smaller incarcerated population and for shorter-term stays (especially in the case of jails)[79] and at a time when the public mental health care system, then comprising largely state-run psychiatric institutions, took more responsibility for the seriously mentally ill than is the case now. Replacing aging jails and prisons creates an opportunity to improve correctional mental health. Better design can reduce the risk of suicide and serious injury in correctional facilities[80] and address the lack of sight and sound privacy that often makes appropriate clinical conversation simply impossible.[81] Better jail design helps understaffed facilities respond to programming demands and allocate staff more efficiently. Jail and prison design, as well as capital investments in brick-and-mortar structures, matters because programming matters.
Reducing recidivism at scale will be a challenge for mentally ill and non–mentally ill offenders alike. Even in cities with well-funded, robustly staffed programs in urban correctional systems, many neighborhoods have very serious crime and substance abuse problems that can easily undermine, upon release, even the most professionally run correctional mental health care program. But when it comes to correctional programs for treating serious mental illness, “nothing works” is not true. Well-run corrections-based programs have shown the ability to increase treatment adherence, reduce adverse outcomes such as violence, and reduce recidivism among mentally ill offenders.[82]
Conclusion and Recommendations
Overall strategy in correctional mental health policy should proceed along two tracks. First, governments should work to shift more responsibility for the most difficult, seriously mentally ill individuals from jails and prisons to the public mental health system. The goal is to fix the “category error” caused by trans-institutionalization. The model is NYC mayor Eric Adams’s effort to expand involuntary psychiatric treatment for unsheltered homeless individuals. That effort is premised on the idea that the public mental health system, not homeless services or the transit system, should be responsible for seriously mentally ill individuals, who are deteriorating because they are not in treatment.[83] Because of Vitek v. Jones, governments cannot directly transfer the victims of trans-institutionalization from jails to psychiatric hospitals. Governments must work more indirectly to fix trans-institutionalization and benefit seriously mentally ill individuals found behind bars instead of in the care of public mental health agencies.
Second, as those plans develop, government should provide humane effective care for seriously mentally ill individuals currently entrusted to correctional systems’ supervision. Outcome measures should focus on reduced recidivism, as well as increased treatment compliance and reduced symptoms relative to seriously mentally ill inmates’ condition at intake. Correctional mental health care is a crucial component of the continuum of care because, without it, people would be sent back into the community system far worse off than in the often-deteriorated condition in which they enter.
Next, we list specific recommendations for reform that operate along these tracks.
1. State governments should assume more responsibility for funding jail-based mental health care. The increased federal burden associated with deinstitutionalization (via enrollment in federal entitlement programs such as Medicaid, Social Security Disability Insurance, and Supplemental Security Income) has been much better understood than the increased burden on localities via correctional mental health care costs. States should provide more funding to local jails for mental health services.[84] States, no doubt, have many claims already on their budgets. But they have shown a willingness to prioritize mental health, such as in the many recent expansions in school-based mental health services and other programs for children. Those expansions represent a prioritization of other populations over the seriously mentally ill.
States can also help with workforce challenges. Long-term correctional mental health professionals who like their jobs often report having entered the field by accident. They learned the satisfactions of the field from experience. One way to increase experience of correctional mental health would be to make serving in a jail or prison a requirement of psychiatric and clinical psychological training programs. That could be done via informal arrangements between communities and local educational institutions. But state governments, because they have control over large state medical schools, would be better positioned to implement such requirements in a systematic fashion.[85] Training programs for psychiatrists and other clinical professionals could require or encourage internships and residencies in jails and prisons.[86]
2. Correctional mental health systems have a special responsibility to the seriously mentally ill and are justified in targeting resources accordingly. The trans-institutionalization thesis holds that government owes a special responsibility to the segment of the incarcerated population who were failed by deinstitutionalization. That logic does not apply to inmates with milder mental disorders that do not qualify as “serious.” In their expansion of correctional mental health programs, some systems have adopted the view that it is a more enlightened approach to focus on “the mental health of all,” and not just “mental illness.”[87] But the idea that “jails are the new asylums” applies only to the seriously mentally ill. All inmates with suboptimal mental health cannot be considered harmed by deinstitutionalization because they would not have been considered for long-term commitment in a previous era. The inmate population with milder mental disorders, who may outnumber those with serious mental illness,[88] may deserve services, as well, but justified as part of correctional institutions’ more general interest in rehabilitating everyone in their custody. When resources—financial, staffing, time spent planning discharge—are scarce, systems are justified in focusing on the seriously mentally ill. State governments’ special responsibility to fund services in local jails should be considered limited to seriously mentally ill jail inmates.
3. Collect, keep, and report better data. Reliable data regarding seriously mentally ill offenders is sorely lacking. In addition to fundamental uncertainty over the prevalence rate, and whether that has changed over time, presumably crucial facts—such as how much jails and prisons spend on correctional mental health care, how many mental health professionals are employed by jails and prisons, and the rate of access to treatment “on the inside”—are also uncertain. The magnitude of deinstitutionalization’s cost shift from state asylum programs to local jails is unknown. In the case of several important data points, old estimates are circulated endlessly in media coverage, amid highly politically charged debates, and can vary significantly.[89] The most commonly cited Bureau of Justice Statistics estimate of the rate of psychiatric disorders in jails and prisons is based on 2011–12 data.[90] It is hard to evaluate different systems and outcomes in different communities. Some programs cultivate a high profile in the media; others, which may be no less effective, are completely obscure, partly because they report little data or outcomes.
4. Repeal Medicaid’s IMD exclusion. Any solution to the so-called criminalization of mental illness in the U.S. will require addressing our nation’s dire shortage of inpatient psychiatric beds.[91] That will require authorizing Medicaid reimbursement for that mode of care through repealing Medicaid’s IMD exclusion. A similar prohibition exists that prevents Medicaid reimbursement in correctional institutions, the Medicaid Inmate Exclusion Policy. Correctional officials have placed more priority on repealing or modifying that prohibition,[92] but, from the perspective of the seriously mentally ill, IMD repeal is more urgent. Since both would increase the cost of an already fiscally burdensome program, IMD repeal should be prioritized.
Progressive reformers argue that correctional health personnel within jails and prisons should enjoy maximal independence from security personnel.[93] This argument raises questions about how security personnel, and correctional agencies more generally, can be held accountable for their obligations if subordinated to another authority. In a psychiatric hospital, security professionals are subordinate to health authorities, not vice versa. Outside that context, it is hard to see how the independence of services for the seriously mentally ill can be appropriately and legally assured. More psychiatric beds, funded by Medicaid, is the most direct route to take to fixing the “category error” of too many people in jails and prisons who would be better served in psychiatric hospitals.
5. Correctional institutions should make more use of long-acting injectables during discharge. Long-acting injectables, in which antipsychotic medications are administrated once a month or so, instead of daily, relieve mental health providers and their seriously mentally ill patients of argument and hassle. Academic studies have established their ability to reduce arrests and rehospitalizations after discharge from psychiatric facilities.[94] They are grossly underused generally[95] and should be made standard practice for high-risk populations such as seriously mentally ill offenders when leaving jail or prison. Long-acting injectables are preferable to the common practice of discharging an inmate with a 30-day supply of medications.[96]
6. Eliminate overuse of administrative segregation; do not abolish it. Correctional institutions have long been criticized for overuse of administrative segregation. In more recent years, that criticism has developed into a movement to abolish it entirely. This movement is a good example of how mental health concerns shape corrections policy more generally. Seriously mentally ill inmates are placed in segregation at disproportionately high rates and are at acute risk of deterioration. Were there fewer seriously mentally ill inmates in custody in jails and prisons, there likely would be less urgency to abolish administrative segregation.
Administrative segregation is not “torture,” as critics sometimes claim, but rather a jail within a jail. Correctional agencies sometimes need to isolate some inmates from others, during both nighttime and daytime hours, because of the need to structure incentives and reduce the potential for violence. Those in the community with a propensity for violence must be isolated, and the same goes for those who are already incarcerated. Agencies can reduce reliance on administrative segregation by investing in programming (which provides “carrots” to take away, for behavioral incentives, rather than using the “stick” of isolation), staff (both medical staff and corrections staff suited by their disposition and training to work with unusually troubled inmates), and infrastructure. Infrastructure investments in spaces featuring natural light and “biophilic” design[97] will address the sensory deprivation associated with traditional administrative segregation. Investing in special mental health housing, and placing inmates in them on a preventive basis, will reduce the need to use extreme forms of isolation. Any system that is reducing the use of administrative segregation should be expanding special housing.
7. Do not use telehealth when reliance on onsite clinical staff is feasible. Much as with remote work, telehealth, though it had been in use before the Covid-19 pandemic, received a large and permanent expansion from that event.[98] Correctional mental health is seen as particularly opportune for telehealth,[99] given the field’s workforce challenges and because of clinical mental health work’s reliance on reported and observed symptoms (e.g., no blood tests). Expanded use of telehealth is a fait accompli and an utter necessity in the many communities where there is no alternative. Telehealth is better than nothing, which is the alternative in some correctional systems. It is not better than anything. The risk is that systems will use telehealth when they do not have to for motivations rooted more in presumed cost savings and convenience than patient health. This could reinforce long traditions of low quality in mental health care, particularly for the seriously mentally ill, and reinforce defeatism in the face of the workforce challenge. If correctional mental health care can be broadly divided into the assessment vs. service provision services functions, the former are more promising for telehealth. Examples include competency and initial classification work during intake. It is less promising for ongoing supervision work and therapeutic work with seriously mentally ill inmates.
Use of telemedicine technology is more common among groups who already have the most access to mental health professionals: the wealthy and educated and households that reside in big metros.[100] The federal Substance Abuse and Mental Health Services Administration hails telemedicine for its potential to overcome barriers in mental health care.[101] The most crucial barriers, when it comes to serious mental illness, have to do with lack of insight or motivation to pursue treatment. Though studies have documented telemedicine’s ability to offset a long-term decline in in-person mental health usage, it is unclear whether part of that effect might simply be a “crowding-out effect”: telemedicine is substituting for, not supplementing, in-person care.[102] Telemedicine can increase the quantity of mental health care, but its effect on the quality of care, for the seriously mentally ill, is more uncertain.[103]
In the corrections context, quality care for seriously mentally ill inmates requires strong relationships between clinical and correctional staff. Those professions differ by gender breakdown,[104] education, and training. Corrections staff value obedience to rules and commands, and their chief priority is security. Mental health professionals value the therapeutic rapport between patients and providers. Mental health professionals experience a “dual loyalty”[105] to their patients, on the one hand; and, on the other hand, to the correctional agency that employs them—and thus, by extension, society. On the inside, medically ethical imperatives such as confidentiality must be balanced against correctional imperatives such as the need to manage assaultive inmates and reduce suicide risk, as well as the practical reality that strict privacy is difficult to maintain in correctional settings. Working relationships between clinical and correctional personnel require mutual respect for their respective professional standards and also informal personal-level habits of trust. That all will be more easily developed through in-person contact.
Appendix 1: Estimating the Rate of Serious Mental Illness in Jails and Prisons
Assessing the seriousness of someone’s mental disorder and his underlying diagnosis can be uncertain in any context because it must be based on symptoms alone, whereas most other health problems’ diagnoses rely on pathologic features (there is no blood test or brain scan for schizophrenia) and/ or etiology (how someone develops schizophrenia is not known with anything like the certainty of how someone develops an infection from a virus).[106] Diagnostic challenges are exacerbated in the corrections context.[107]
Correctional systems are decentralized. The state and localities that run them vary in how they track and report rates of mental disorders. Estimates of serious mental illness can vary even within jail systems in the same state.[108] Commonly, correctional systems categorize inmates based not their underlying disorder but on what kind of services or accommodations they need.[109] This can entail a certain circularity: someone is considered seriously mentally ill because he qualifies for specialized housing programs that are reserved only for those with a serious mental illness. A jail might categorize one schizophrenic inmate in its most acute category if his behavior requires specialized housing while other inmates with that same diagnosis whose behavior is more stable may be placed in the general population. Another administrative designation might be those who receive antipsychotic medication. Jails and prisons have long been criticized for overreliance on medications to sedate inmates.[110] To the degree that that is true, it could inflate estimates of serious mental illness in jails and prisons.
Many correctional systems have, in recent years, expanded their mental health staff and instituted new training programs for all staff, such as de-escalation, that emphasize heightened attentiveness to mental health concerns.[111] That could lead to more identification of mental disorders than in the past. Heightened adoption of accreditation standards, in order to anticipate or respond to lawsuits, may have led to more cases getting picked up. Abolitionists’ belief that many inmates are sick, not criminals, could create pressure to keep rates high or blur the line between serious mental illness and the more common, functional illnesses. Systems have faced lawsuits over suicides and other adverse outcomes and are therefore highly concerned about not overlooking anyone potentially at risk.
Press reports regularly conflate functional mental disorders (which afflict 25% of the general population and over 50% of the incarcerated) with serious mental illnesses (which afflict less than 10% of the general population and 15%–20% of the incarcerated [Table 1]).
Appendix 2: Mental Illness and Violence
The most straightforward explanation for why the seriously mentally ill are incarcerated at a disproportionately high rate is that seriously mentally ill people, especially when not in treatment, are disproportionately violent. A substantial body of research supports the notion of a link between untreated serious mental illness and violence.[112] The federal government estimates that 15 million American adults are seriously mentally ill and that one-third, or 5.2 million, received no treatment in the past year.[113] Other estimates peg the nontreatment rate at as high as 50%.[114] Because the public mental health care system is incapable of pushing the rate of treatment higher, it is unsurprising that the criminal justice system should bear so much responsibility for the care and treatment of serious mental illness.
Still, many object to the idea of a connection between mental illness and violence.[115] Table 3 presents six common arguments that attempt to de-link violence and mental illness, with responses to each.
Table 3
Responses to Common Arguments Attempting to De-Link SMI and Violence
| Critics’ Argument | Response |
| 1. Mental disorders are common. One-quarter of the adult population has them,[116] a population far too large to be violent. | The core claim concerns the link between serious mental illness, especially when untreated, and violence. The seriously mentally ill are a subset of the larger universe of adults with mental disorders. |
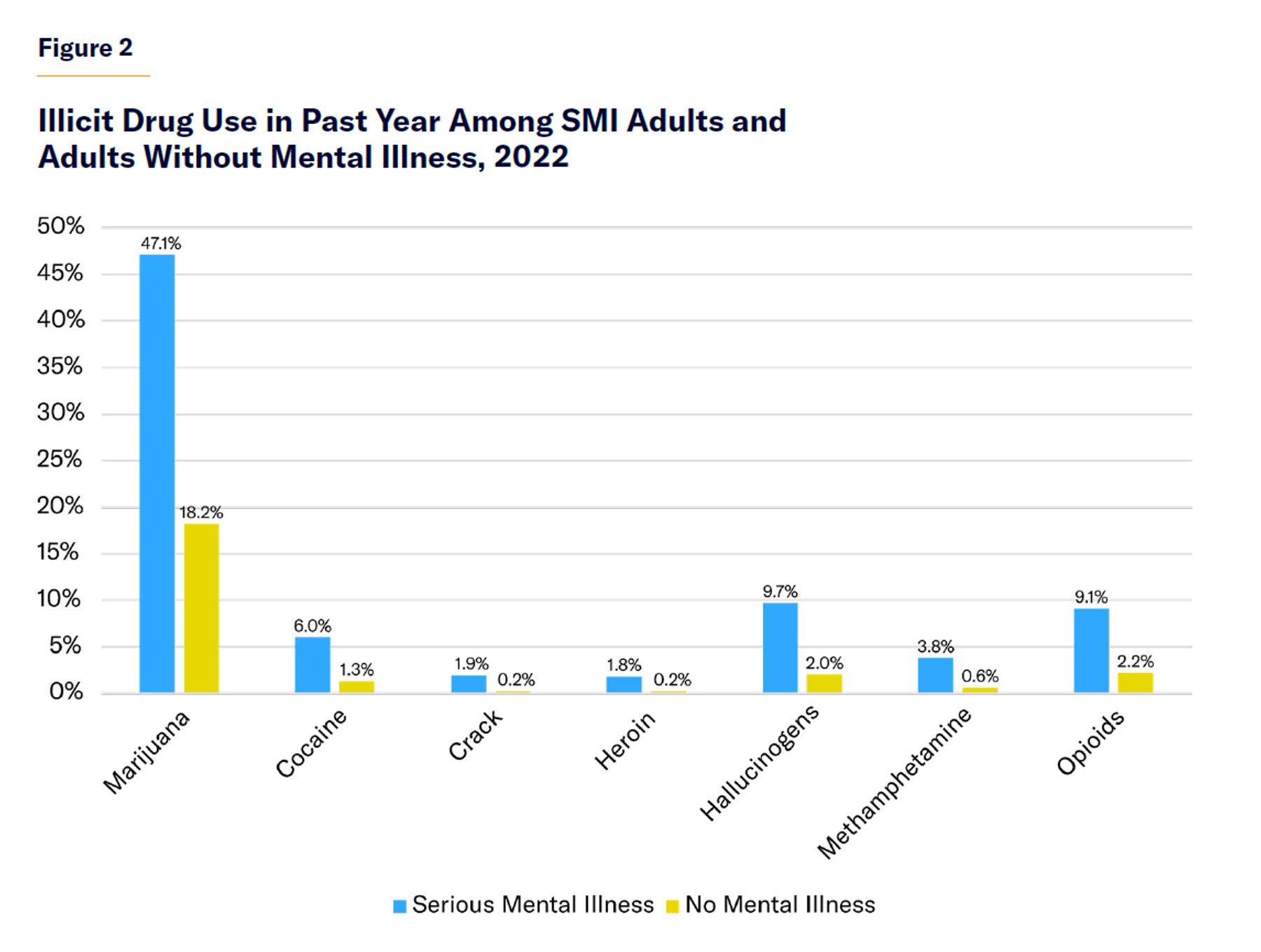
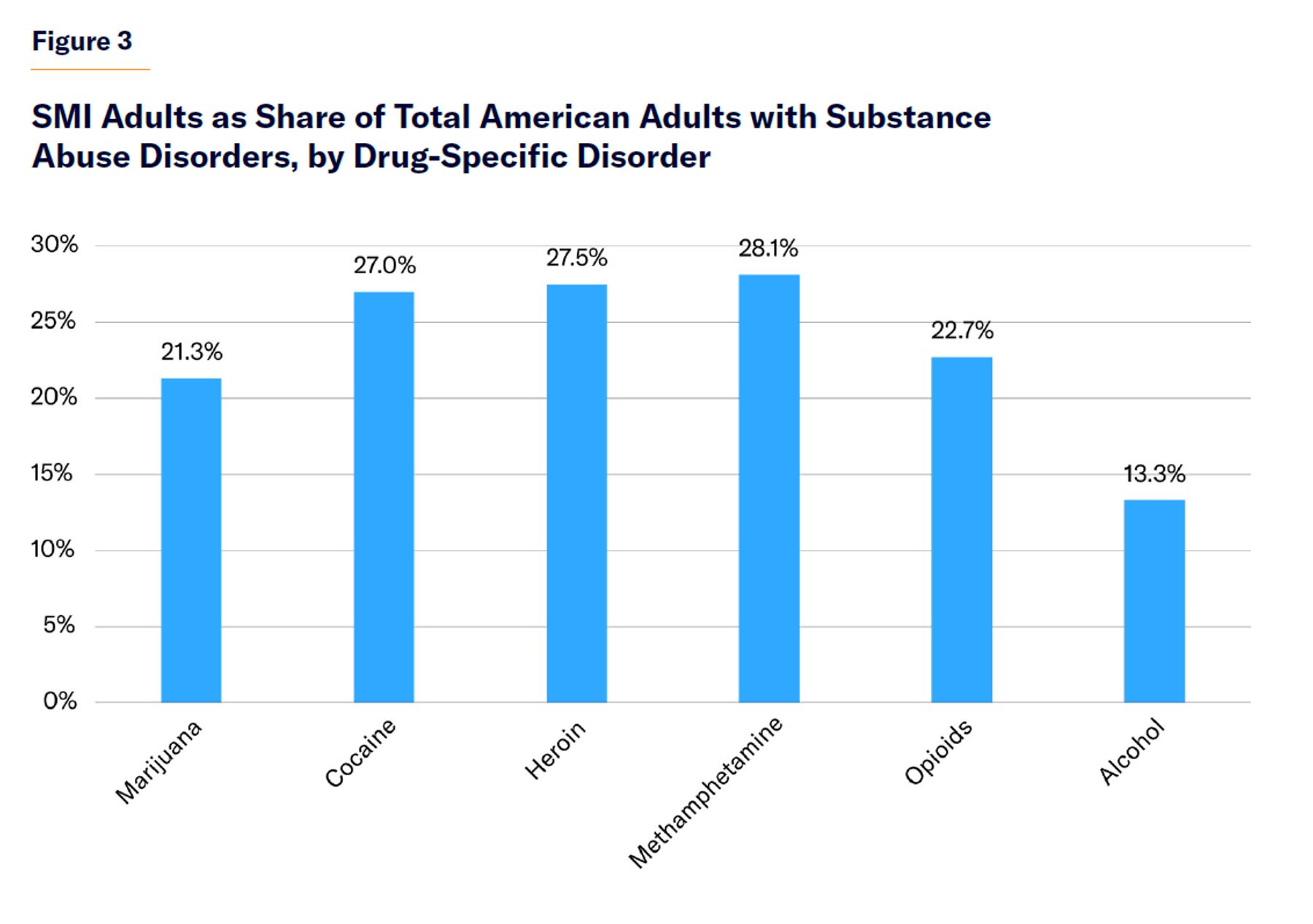
| 2. The problem is substance abuse, not mental illness. | Substance abuse is indeed a major risk factor for crime and violence.[117] According to Homer Venters, former chief medical officer for the NYC jails system, “ Substance use disorder is the most common diagnosis in correctional health.”[118] Substance abuse can lead to criminal offending by increasing aggression or making people unresponsive to social norms and the informal mechanisms by which civil society regulates behavior. But seriously mentally ill people use illicit drugs at disproportionately high rates (Figure 2),[119] which therefore places them at an elevated risk of crime and violence. Though their share of the adult population is only about 6%, they constitute 20%–30% of adults with drug abuse disorders (Figure 3). |
| 3. Violence caused by serious mental illness is real but rare. | The seriously mentally ill are associated with certain kinds of violence. For example, interfamily violent acts and mass shooting are disproportionately committed by people with serious mental illness.[120] But they are also, generally, more violent than the rest of the population. According to the Bureau of Labor Statistics, “Psychiatric technicians and aides have some of the highest rates of injuries and illnesses of all occupations.”[121] |
| 4. Violence committed by seriously mentally ill individuals is a small percentage of total violent crime. | The core claim of those concerned with the link between serious mental illness and violence does not concern whether seriously mentally ill people commit all, or even most, crime, but whether they commit a disproportionate share of it. |
| 5. The seriously mentally ill are more likely to be victims than perpetrators of violence.[122] | This is not a response to the core claim. The core claim is that people with untreated serious mental illness wind up incarcerated at a disproportionately high rate partly because people with untreated serious mental illness are disproportionately violent. A group can be, relative to the general population, both more likely to be victimized and more likely to be perpetrators of violence. That is the case with the seriously mentally ill. Some studies have even cast doubt on whether they are more at risk of being victims of violence.[123] |
| 6. The seriously mentally ill are incarcerated at a high rate because they fail to comply with correctional facilities’ rules, which leads to infractions and longer detentions than their (often low-level) charges would ordinarily justify.[124] | This “vortex” effect happens,[125] but it is unclear how big of a problem it is. The rate of serious mental illness in jails has remained high, and even risen, in systems such as NYC, which have drastically reduced incarceration for low-level offenses.[126] |
About the Author
Stephen Eide is a senior fellow at the Manhattan Institute and contributing editor of City Journal. He researches social policy questions such as homelessness and mental illness. Eide has written for many publications, including National Review, New York Daily News, New York Post, and Wall Street Journal. His first book, Homelessness in America: The History and Tragedy of an Intractable Social Problem, was published in 2022. He was previously a senior research associate at the Worcester Regional Research Bureau. Eide holds a B.A. from St. John’s College in Santa Fe, New Mexico, and a Ph.D. in political philosophy from Boston College.
Acknowledgments
The author would like to thank Brandon Fuller, Hannah Meyers, Rafael Mangual, and Carolyn Gorman for their feedback. He would also like to thank Sergeant Chuck Hardy and his colleagues at the Lane County (Oregon) Sheriff’s Office for hosting a visit to the Lane County Jail.
Endnotes
Photo: Hans Neleman/Stone via Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).