The Anatomy of Institutional Capture Gender Medicine Policy and the Texas Medical Association

Photo: A-Digit / DigitalVision Vectors via Getty Images
Executive Summary
- The politicization of the Texas Medical Association (TMA) has been evident since at least 2016, when members of the Medical Student Section introduced Sexual Orientation Change Efforts in Minors. But it accelerated in 2020 with the creation of TMA’s LGBTQ Health Section. In 2021, TMA modified its bylaws to expand the LGBTQ Section’s mission to include “educat[ing] policymakers and advocat[ing] for policies addressing the medical spectrum of gender identity to improve access to quality health care.”[1] This change introduced tension between TMA’s ostensible commitment to evidence-based policies and political considerations.
- LGBTQ Section members with intellectual conflicts of interest have served on reference committees tasked with evaluating resolutions related to gender-affirming care, which is significant because data from 2022 reveal that roughly 92% of all resolutions recommended for adoption by a reference committee were ultimately adopted by TMA’s House of Delegates (HOD).[2]
- LGBTQ Section members discussed ways to “Trojan horse” unpopular policies through TMA’s HOD by using deceptive language and distancing themselves from certain resolutions by asking medical student members to introduce them.
- In 2022 and 2023, TMA members expressed concerns to executive leadership about conflicts of interest among board members, arguing that TMA’s embrace of social-justice activism did not fairly represent the interests of members, who are primarily concerned with issues of “scope, tort, and autonomy,” according to surveys. They also raised concerns about a possible breach of the fiduciary duty that TMA board members owe other members. TMA’s board of trustees failed to address their concerns.
- In 2025, a resolution to create an ad hoc committee to study TMA’s gender-affirming-care policies received overwhelming support from TMA members in online testimony provided to the 2025 Reference Committee on Science and Public Health. Seventeen TMA members testified in favor, and only three testified against. Nevertheless, the 2025 Reference Committee recommended not to adopt the resolution. Three of the six members constituting the 2025 Committee possessed clear intellectual conflicts of interest as LGBTQ Section members, or as cohosts of TMA’s Continuing Medical Education course “Transgender Healthcare.”[3]
Introduction
In the Supreme Court’s recent 6–3 ruling upholding Tennessee’s law prohibiting minors from accessing medical interventions for the treatment of gender dysphoria, Justice Clarence Thomas’s concurring opinion shed light on the role that medical societies have played in creating the illusion of consensus around so-called gender-affirming care: “There are particularly good reasons to question the expert class here, as recent revelations suggest that leading voices in this area have relied on questionable evidence and have allowed ideology to influence their medical guidance,” Thomas wrote.[4]
For many Americans beginning to pay closer attention to this issue, it may seem backward for a Supreme Court justice to question the expertise of U.S. medical associations. But as the Skrmetti ruling and a Department of Health and Human Services (HHS) report on pediatric gender dysphoria[5] make clear, these organizations are primarily trade associations that lobby for their members’ interests—not impartial arbiters of scientific information.
Moreover, medical associations are susceptible to institutional capture.[6] As the HHS report notes, medical associations tend to defer to highly specialized subcommittees when crafting policy on novel issues like medical treatment for pediatric gender dysphoria.[7] Members of these subcommittees tend to be ideologically aligned and may have conflicts of interest that can bias professional judgment or compromise research integrity.[8] These conflicts of interest can be financial or intellectual, stemming from commitments to ideas, beliefs, or scholarly activities that can bias objectivity even in the absence of material incentives.[9] Support for gender affirmation is not seen as an intellectual conflict of interest but rather as a mark of expertise. However, calls for caution and additional safeguarding are often cast as veiled discrimination.
This report reviews dozens of resolutions, reports, policies, and never-before-published internal correspondence to provide a high-resolution look at the internal politics of the Texas Medical Association (TMA), a state affiliate of the American Medical Association, with more than 55,000 physician and medical student members. It offers a case study in institutional capture, revealing the incentives and group psychology that have led nearly every major medical association to endorse gender-affirming care.[10]
Materials and conversations with TMA members allowed me to reconstruct a timeline that sheds light on how TMA came to adopt highly ideological policies on affirming care. These policies directly undermine principles of evidence-based medicine, the stated priorities of rank-and-file TMA members, and the organization’s stated ethos of serving the people of Texas and preventing and curing disease.
Despite the Texas legislature’s determination that affirming-care interventions should be prohibited for scientific and ethical reasons,[11] recent medical practice reversals abroad, the HHS report on pediatric gender dysphoria, and the Supreme Court’s Skrmetti ruling, TMA’s position on the issue remains unchanged. The organization says that it supports “the practice of evidence-based, patient-centered, gender-affirming care and will aggressively oppose the use of potentially harmful, unproven therapies for children.”[12]
TMA presents its support for gender-affirming care not merely as a matter of medical science but of civil rights. Its embrace of the civil rights framing accelerated in 2020, when TMA established an LGBTQ Health Section, which ultimately received a voting member in TMA’s House of Delegates (HOD). Members of the section—which was formed to support LGBTQ-identifying physicians—came to be seen as de facto experts on transgender health care. Many of them went on to occupy high positions within the association, including as members of influential committees and councils that review and establish TMA policy.
LGBTQ Health Section members have been able to wield outsize influence on these committees, where policy recommendations are often voted through without formal debate, unless they are “extracted” for further debate on the house floor.[13] Moreover, correspondence between LGBTQ Health Section members reveals what one member described as an attempt to “Trojan horse”[14] policies through TMA’s HOD. Other members have complained to leadership about these activists’ influence on councils, committees, and the board itself, but the association has failed to adequately address these concerns or to initiate governance and oversight reform. Similarly, efforts to reform TMA’s gender medicine policies from within, using the policymaking channels available to members, have been subverted by institutional capture.
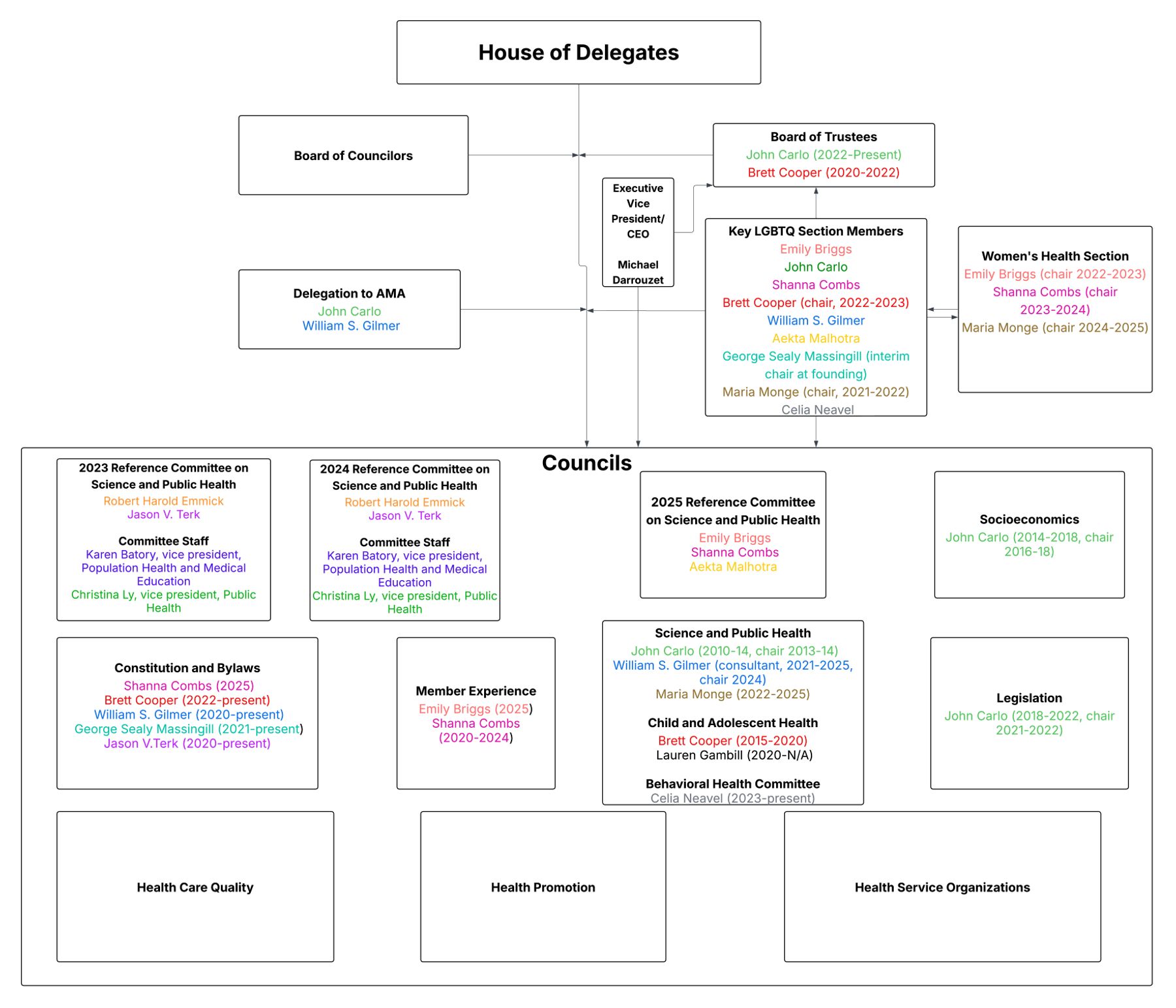
Background on TMA’s Organizational Structure
TMA’s primary policymaking body is HOD, comprising nearly 600 delegates elected by local county medical societies, sections, and other constituencies. It meets annually at TMA’s conference, TexMed, to elect leaders, establish policies, and present awards. Between annual meetings of HOD, the board of trustees serves as the executive authority, with the two forming the core of the governance structure.
Supporting this governance structure are three main types of advisory bodies:
- Councils: Broad policy groups that study issues in key domains (e.g., legislation, public health, science, socioeconomic issues) and make recommendations to HOD or the board
- Committees: Focused, task-specific groups that handle narrower issues and provide expertise and recommendations
- Sections: Membership subdivisions that represent specific constituencies within the association (e.g., LGBTQ members, residents, young physicians, women physicians) and give those groups a voice in TMA governance
TMA Gender Medicine Policy Timeline
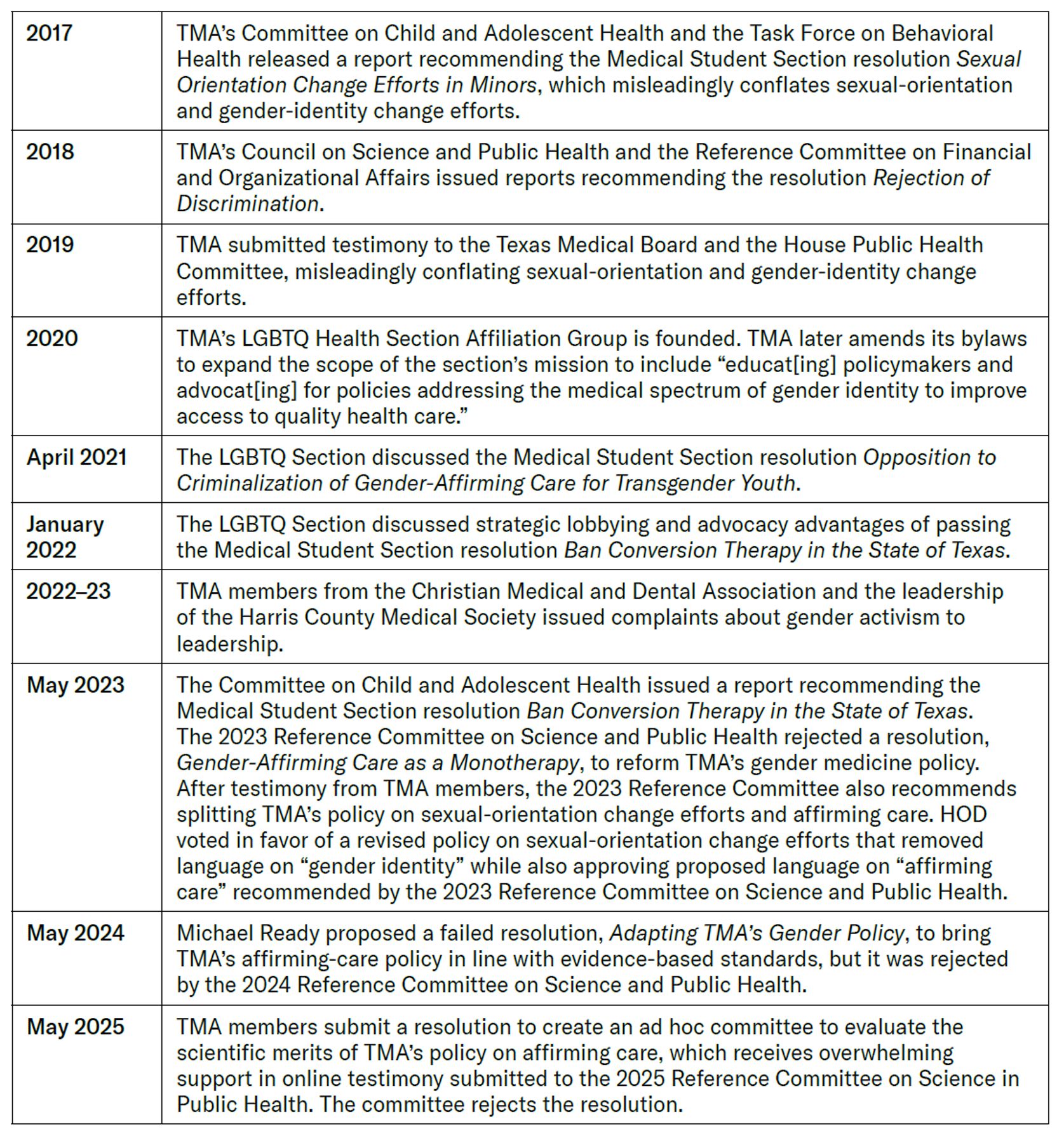
Table 1 provides an overview of changes in TMA’s approach to gender medicine. Next, I will elaborate on the key turning points.
Table 1
Timeline of TMA’s Approach to Gender Medicine
2016–17: Sexual-Orientation Change Efforts in Minors
In 2016, when TMA had no policies specifically addressing pediatric medical transition, the Medical Student Section introduced a resolution, Sexual Orientation Change Efforts in Minors.[15] The proposed resolution asserted that TMA should “advocate for legislation banning conversion therapy for patients under 18 years of age.”[16] After being referred to two of TMA’s “expert” committees for evaluation, the resolution was expanded to cover not only sexual-orientation change efforts but also gender-identity change efforts.[17]
TMA’s Committee on Child and Adolescent Health and the Task Force on Behavioral Health issued a report on the resolution, citing a 2015 SAMHSA report on “conversion efforts” that reviewed research only on sexual orientation. Nevertheless, authors of the TMA report misleadingly claimed that the same research applied to gender identity.[18]
As a result, the expert committees recommended the policy and expanded its language: “The Texas Medical Association supports treatment and therapies rooted in acceptance and support regarding an individual’s sexual orientation and gender identification.” Confusingly, the resolution was still limited to opposition to “practices aimed at changing an individual’s sexual orientation, including conversion therapy” (emphasis added).[19]
TMA claims to endorse “evidence-based” therapies, but its conflation of sexual-orientation change efforts and gender-identity change efforts is not based on evidence. Indeed, as psychologist and expert witness James Cantor noted regarding a similar claim advanced by the American Academy of Pediatrics in its 2018 position statement,[20] “studies of conversion therapy have been limited to sexual orientation, and, moreover, to the sexual orientation of adults, not to gender identity and not of children in any case.”[21] Remarkably, despite the lack of evidence for the harms of gender-identity change efforts, TMA’s “experts” on the Committee on Child and Adolescent Health and the Task Force on Behavioral Health assert that anything short of affirmation is “coercive and likely harmful.”[22]
In a sign of things to come, the report also notes that “[TMA] members stated that seeking legislation [on conversion therapy] would be a concern for the association, as the topic would be so politically controversial that it would undermine other TMA efforts.”[23]
2017–18: TMA’s Rejection of Discrimination Policy
In 2017, the Young Physician Section, Resident and Fellow Section, and the Medical Student Section of TMA’s HOD introduced a resolution calling on TMA to adopt a policy “opposing any discrimination based on an individual’s sex, sexual orientation, gender identity, race, religion, disability, ethnic origin, national origin, or age.”[24]
The resolution noted that LGBTQ individuals have higher rates of psychiatric disorders, substance abuse, and suicide and that trans-identified individuals have higher rates of mental-health diagnoses and suicide. These are explained through a “minority stress” framework, which takes for granted that health disparities are the product of discrimination or stigma, including discrimination in health-care access. The resolution fails to acknowledge any criticism of the “minority stress” theory, the most compelling of which argue that self-reports of discrimination are confounded by mental-health status and stem from cognitive and processing biases associated with psychiatric disorders.[25]
TMA’s Reference Committee on Science and Public Health was tasked with evaluating the initial resolution in 2017. The Reference Committee recommended the resolution for adoption and proposed an additional amendment calling on TMA’s Council on Science and Public Health to “provide recommendations to guide TMA activities related to gender and sexual diversity.”[26]
TMA’s HOD referred the resolution to the Council on Science and Public Health, which, in 2018, coauthored a report with George Sealy Massingill, who was chosen by the council to chair a new LGBTQ working group. The report uncritically accepted the minority stress framing and emphatically recommended the resolution for adoption.[27] It went a step further by encouraging “physician efforts” to incorporate protections for gender identity into “their practices, medical schools, hospitals, and clinics.”[28] Significantly, the report cites an Obama-era federal rule, which both interpreted Section 1557 of the Affordable Care Act to include protections for gender identity and deemed restrictions on gender transition as discriminatory,[29] thus helping set the stage for later TMA policy.
In 2018, TMA’s Reference Committee on Financial and Organizational Affairs recommended the resolution and report for adoption.[30] Because none of the proposed amendments was extracted beforehand, the full HOD never debated the policy, and it was approved as part of a larger block vote with other resolutions.
In testimony submitted to the Reference Committee, TMA’s Council on Science and Public Health advocated for the creation of a committee to address “the health issues of LGBTQ populations,”[31] which would culminate in the founding of TMA’s LGBTQ Health Section in 2020.
2019: TMA Submits Testimony to the Texas Medical Board and the House Public Health Committee
Despite the conflation of sexual-orientation change efforts and “gender-identity” change efforts in the lead-up to TMA’s adoption of its policy Sexual Orientation Change Efforts in Minors, the policy ultimately asserts that TMA opposes practices aimed only at changing an individual’s sexual orientation. TMA’s advocacy arm quickly stretched the scope of this policy to gender identity.
In doing so, it followed a familiar script. For example, in its 2018 policy statement on gender transition in minors, the American Academy of Pediatrics cites research on homosexuality in adults when asserting that a child’s incongruent gender identity is immutable.[32]
In 2019, the American College of Pediatricians (ACPeds) petitioned the Texas Medical Board to discourage medical interventions for trans-identified youth in favor of counseling services and psychotherapy. Then-TMA President Dr. David Fleeger submitted testimony to the Texas Medical Board opposing the recommendation on the grounds that it would allow for “conversion therapy”[33]—even though TMA policy at the time prohibited conversion efforts only for sexual orientation. Fleeger claimed that TMA’s stance reflected “evidence-based care . . . for all children . . . including those who do not identify with the sex they were assigned at birth.”[34]
Despite the earlier concession from expert committees that seeking legislation on conversion policies could divide TMA members and undermine other issue priorities, in May 2019 TMA provided written testimony in support of HB517,[35] which would have made conversion efforts, including attempts to change gender identity, illegal in Texas. In its written testimony, TMA accepted HB517’s assumption about the immutability of gender identity and once again misleadingly conflated sexual-orientation change efforts with gender-identity change efforts.
2020: Founding of LGBTQ Health Section Affiliation Group and Amending TMA’s Bylaws
In 2020, in response to pressure from TMA’s LGBTQ Health Workgroup, the board approved the creation of a new permanent member section, the LGBTQ Health Section.[36] Because this change required amendments to TMA’s bylaws and constitution, the board directed the Council on Constitution and Bylaws to draft an amendment formally establishing the LGBTQ Health Section and giving it a formal voting member in HOD.
The amendment was drafted by then-chair of the Council on Constitution and Bylaws, William Gilmer, who would become a prominent member of the LGBTQ Section. It describes the section as an affiliation group open to “all members,” which would “study and advance the scientific basis for the care of LGBTQ patients,”[37] as well as “develop policy and resources on LGBTQ health and advance evidence-based scientific information on the care of LGBTQ patients.”[38]
The creation of the LGBTQ Health Section did not follow standard TMA procedure for modifying its constitution, which requires ratification at two consecutive TMA sessions. In 2020, with HOD suspended due to Covid-19, TMA’s board of trustees functioned as a Disaster Board. The Disaster Board invoked its exceptional authority and accepted an amendment to Article V of TMA’s constitution, allowing for an LGBTQ Section representative to join HOD, although the policy still required ratification by HOD the following year. In the interim, the Council on Constitution and Bylaws recommended adopting “an amendment to Chapter 3 of the Bylaws,” which would “allow the LGBTQ Health Section to begin the process of establishing the section, including the formulation of its operating procedures.”[39]
An additional amendment to TMA’s bylaws in 2021 expanded the scope of the LGBTQ Section’s mission, which would now involve “educat[ing] policymakers and advocat[ing] for policies to improve access to quality health care.”[40] By introducing political commitments, this amendment created obvious tension with the association’s commitment to evidence-based principles, with the former eventually supplanting the latter.
While the LGBTQ Health Section does not have decision-making authority, its members have come to occupy high positions within TMA’s councils and committees, allowing them to shape TMA’s policymaking process. Despite being originally characterized as simply an “affiliation” group—one that is recognized because of the personal characteristics of its physician-members—TMA’s website states that the section is responsible for “communicat[ing] TMA policy and expertise on LGBTQ health to other physicians, policymakers, and the public.”[41] I.e., the scientific “expertise” of the section was assumed to flow naturally from the fact that its members identified as LGBTQ.
The creation of the LGBTQ Health Section represents a turning point in TMA’s mission. Now considered the de facto “experts” on LGBTQ issues by the broader TMA, the section would push the organization toward increasingly activist positions and strategies that diverged from evidence-based medicine and, very likely, from the priorities of many rank-and-file TMA members.
2021: Opposition to Criminalization of Gender-Affirming Care for Transgender Youth
Presumably in response to growing state-level legislative activity regulating pediatric gender medicine, LGBTQ Section members began considering ways to fortify TMA’s policies on affirming care.
In April 2021, TMA’s LGBTQ Section met to discuss a controversial resolution, Opposition to Criminalization of Gender-Affirming Care for Transgender Youth, set to be heard by TMA’s HOD the following month. The resolution, which would update TMA’s Sexual Orientation Change Efforts in Minors policy, stated: “TMA supports physician efforts to provide medically appropriate therapies affirming gender identity and opposes the criminalization of these practices.”[42] Ultimately, this policy passed and resulted in a new provision added to the sexual-orientation change efforts policy, which was also strategically renamed Sexual Orientation Change Efforts and Gender-Affirmation Therapies for Minors.[43]
The LGBTQ Section’s April 2021 discussion of this resolution is emblematic of how a small but well-coordinated group of activist members was able to influence TMA policies by taking advantage of its organizational structure and procedural mechanisms, outside the view of TMA’s HOD. The resolution was also introduced by TMA’s Medical Student Section.
At the time, TMA had already passed broad nondiscrimination policies, including protections for gender identity, as well as other policies related to improving LGBTQ health-care access and LGBTQ education in academic health centers.[44] But the only policy on the books that even indirectly covered treatment of pediatric gender dysphoria was the 2016 resolution Sexual Orientation Change Efforts in Minors, introduced by the Medical Student Section.[45]
Given the limits of that policy, the LGBTQ Section was highly motivated to push through new policies via what some members described as a “Trojan horse.”[46] In particular, their goal was to craft policy that would force TMA’s Council on Legislation to pursue its preferred agenda. As Massingill put it at the April 2021 meeting,“If you have policy that clearly defines what the Council on Legislation should be doing, you can complain when they don’t do it . . . so having clear policy is always better.”[47] In 2024, Massingill would cohost TMA’s Continuing Medical Education event on transgender health care,[48] while continuing to serve on the influential Council on Constitution and Bylaws, for which he is currently vice-chair.[49]
Also in attendance at the meeting was TMA board member Brett Cooper, an affirming-care gender clinician for children and adolescents, who had previously worked at the GENECIS gender clinic for adolescents,[50] jointly run by the University of Texas Southwestern Medical Center and Children’s Medical Center Dallas, before it was shut down in November 2021. Although the section was adamant about supporting the measure, Cooper shrewdly recognized that the original policy addressed sexual orientation only in the title. Although TMA has already begun taking bolder stances opposing “gender identity change efforts,” Cooper and other members were aware that the existing policy on sexual-orientation change efforts was limited in scope and were eager to expand its reach to “gender identity.” Cooper wanted the authors to make clear in the text of the resolution that it includes “opposition to both sexual-orientation and gender-identity change.”[51]
Cooper is presently being sued by Texas Attorney General Ken Paxton for violating SB14,[52] which prohibits sex-rejecting procedures for minors. The complaint in that lawsuit includes a social media post in which Cooper advertises that he once encouraged a minor patient, a trans-identified female, to move out of her parents’ home and become legally emancipated.[53] The lawsuit also alleges that Cooper falsified diagnoses and billing codes in violation of the False Claims Act. As a result, Cooper has signed a Rule 11 agreement that prevents him from practicing medicine.[54] Nevertheless, Cooper’s star has not dimmed within TMA. On the contrary: he was reappointed to TMA’s Council on Constitution and Bylaws in May 2025.[55]
In the same April 2021 meeting, Maria Monge—a pediatrician who held a fellowship in adolescent medicine at Boston Children’s Hospital when it was the epicenter of youth gender medicine—suggested that TMA’s Committee on Child Adolescent Health agreed that policy should be expanded to explicitly include a prohibition on gender-identity change efforts.
Notably, LGBTQ Section members seemed reluctant to openly champion the policy themselves and preferred to have medical student members testify in support. Indeed, the LGBTQ Section requested that medical student members submit testimony to the Reference Committee on Science and Public Health in their capacity as student members rather than as LGBTQ Section members. “If one or several of our medical students wanted to draft some online testimony, let us review that at some relatively short future point and get that into the online refcom [Reference Committee on Science and Public Health] testimony,”[56] Massingill declared to fellow section members.
Emily Briggs—a founding member of the LGBTQ Section who would also go on to cohost TMA’s CME on Transgender Healthcare—then revealed that she would be chairing the 2021 Reference Committee on Science and Public Health that was set to evaluate this policy.[57] Not surprisingly, the reference committee under Briggs recommended the resolution for adoption and the policy was added to TMA’s policy compendium.
TMA’s Reference Committee on Science and Public Health, whose members are chosen each session by the speaker of HOD, is tasked with reviewing and recommending resolutions for the House to consider. The House almost always defers to their recommendations: in 2022, 92% of resolutions recommended for adoption by a Reference Committee that year were ultimately adopted by the House.[58]
Another prominent participant in the April meeting was John Carlo, a physician from the Dallas County Medical Society who, at the time, served on TMA’s Council on Legislation, which lobbies for state legislation consistent with TMA priorities. Carlo updated members of the LGBTQ Section about behind-the-scenes efforts that the association was taking regarding SB 1646, which would have classified sex-trait modification as “child abuse,” and SB 1311, an early attempt to prohibit minors from accessing these procedures. Members could rest assured that, even if they didn’t see any publicly visible lobbying from TMA,“that doesn’t mean that there’s not some things that are going on behind the scenes to try to get these bills killed. Sometimes it’s better not to blow oxygen into the fire, so to speak,”[59] explained Carlo. SB 1311 eventually died in the House Public Health Committee.
In May 2021, Carlo became chair of the Council on Legislation.[60] One year later, he joined TMA’s board of trustees as an at-large member, where he remains to this day.[61] Carlo has also been appointed to influential councils on science, public health, and socioeconomics.
Since 2012, Carlo has also served as CEO of Prism Health North Texas,[62] a large community-based health organization specializing in LGBTQ primary-care services, including endocrine and surgical affirming care for adults.[63] While structured as a 501(c)(3), Prism generates over $125M annually, primarily through fee-for-service billing.[64] In 2024, public records show that Carlo received $405,146 in compensation.[65] Prism has expanded in recent years and now owns tens of millions of dollars in real estate in the Dallas–Fort Worth area.
Carlo has held influential policymaking roles within TMA and the American Medical Association (AMA), on whose Council on Science and Public Health he recently served.[66] However, he does not appear to have reported any conflicts of interest stemming from his participation in these roles while also serving as CEO of Prism Health, which stood to benefit financially from expanded access to gender-affirming care in the state.
2022: Banning “Conversion Therapy”
In January 2022, the LGBTQ Section discussed another resolution introduced by TMA’s Medical Student Section, Banning Conversion Therapy in the State of Texas.[67] The resolution aimed to clarify TMA’s stance on “conversion therapy” by explicitly including gender identity and not just sexual orientation. Unlike past iterations, this policy explicitly defines conversion therapy as an attempt to change gender identity and also asserts that the TMA opposes efforts to legalize conversion therapy. Massingill explained that this resolution was important because it “actually forces the advocacy staff to say we have a position.” In Massingill’s view, it was important that the LGBTQ Section “PRESS them to take a position, because it’s pretty clear they don’t always want to do the right thing.”[68]
What stands out most from the January 2022 deliberations is the tactics that section members used to achieve their goals. To avoid the perception that the LGBTQ Section was the sole champion of these causes, leaders encouraged TMA medical student members to craft resolutions and supply testimony. Some LGBTQ Section members, such as Maria Monge, thought that older physicians would be less likely to oppose resolutions and testimony coming from junior members: “I love that you all can put up often sometimes the more controversial things. . . . People are much more willing to listen because they’re coming from the medical students, right?”[69]
In the January 2022 meeting, the section discussed ways to use deception to force TMA’s lobbying arm to defend gender-affirming care in Texas without attracting scrutiny. According to Massingill, one way would be to use “the right Trojan horse”—i.e., a policy that, on its face, would say little about controversial issues but that, in practice, could be interpreted to require gender-affirming care.
Dr. Brett Cooper, then on TMA’s board of trustees, offered a proposal that he said was inspired by the former medical director of his gender clinic. Cooper suggested that they push for a policy that simply says that the TMA opposes “efforts by nonphysicians . . . hospital[s] or health system[s] to interfere in the practice of evidence-based medicine.”[70] As long as they could get TMA to endorse the view that gender-affirming care was evidence-based, this policy would have the effect of disallowing any efforts to interfere with it.
Later in 2022, TMA’s Council on Socioeconomics issued a report recommending a resolution, Protections Against Interference in the Practice of Medicine and the Patient–Physician Relationship,[71] which was very similar to the policy proposed by the LGBTQ Section.[72] Ultimately, this became official TMA policy after a block vote in HOD. Meanwhile, the policy on banning “conversion therapy” was referred to TMA’s Committee on Child and Adolescent Health for further evaluation.
LGBTQ Section minutes that were later legally acquired by a TMA member did not match the contents of the discussion as recorded by a section member.[73] The minutes of the meeting that were provided failed to mention any discussion of the policy on banning “conversion” therapy and failed to mention that the policy on noninterference in medical practices was presumably designed as a “Trojan horse” to protect affirming care.
2022–23: Internal Calls for Reform
As a 501(c)(6) organization—a nonprofit trade association—members of the TMA’s board of trustees have fiduciary obligations, legal and ethical, to the organization.[74] Members of the board are to promote the “best interests” of the TMA and its members. In 2022, however, some TMA members began to voice concerns about the inclusion of Drs. Cooper and Carlo on the board of trustees and TMA’s embrace of advocacy efforts that did not match broader member priorities.
One member of the board of trustees—who preferred not to be named for this report—initially assumed that TMA leadership would be eager to address these complaints. This trustee tried to push the board to implement governance reform, including mandatory conflict-of-interest disclosures, section and committee transparency, and policy audits. The board, however, seemed unwilling or unable to take any steps to mitigate institutional risk—a reflection of paralysis, at best, or a breach of fiduciary duty, at worst. After speaking out, the trustee’s reputation was attacked, which effectively silenced the trustee.
In May 2022, 60 TMA members from the Christian Medical and Dental Association sent a letter to then-TMA president Linda Villareal, criticizing the organization’s increasingly unscientific and bold stance on pediatric gender medicine.[75] The letter criticized TMA for public statements that conflict with “the long-held standards of TMA and objective, evidenced-based, Hippocratic medicine.”[76] It also took issue with TMA claiming to speak on behalf of its 55,000 members when issuing briefs or public announcements on pediatric gender medicine. Their concerns went unanswered by President Villareal and then–executive vice president and CEO Michael Darrouzet.
In October 2023, leaders from the Harris County Medical Society (HCMS), which constitutes nearly 25% of TMA membership, sent a letter to Darrouzet thanking him for holding a meeting in which members were able to voice concerns about activism within TMA, including from the board.[77]
The letter noted that many of these concerns had already been expressed in May 2022 and had yet to be addressed. But optimism remained: “Overall, we look forward to our concerns being addressed by the Board. We believe this will demonstrate to our members that TMA cares and listens to their concerns, ensure proper alignment of legislative priorities with the membership’s priorities, and reform the governance, disclosure, oversight, and responsiveness of the TMA.”[78] HCMS’s concerns were more fully explained in a 2023 memo regarding items to be discussed with TMA leadership. According to the memo, HCMS members felt that their priorities were being ignored, while a “powerful gender-affirming lobbying bloc is biasing the TMA agenda away from our broader, stated mission.”[79]
The HCMS memo referenced the results of a survey conducted by TMA’s Justice, Equity, Diversity and Inclusion (JEDI) task force on member priorities, which found that only 1% of TMA members believed that affirming care was among the top organizational priorities, and less than 25% agreed that it was “important broadly.”[80]
In 2024, trustee Kim Monday—who now chairs the board[81]—reportedly opted not to promote the findings of that survey that she had helped organize as cochair of the JEDI taskforce because the findings undermined Monday’s sense of member priorities. In a text message to members of the LGBTQ Health Section, Monday wrote: “I personally pushed for that survey because I believed our organization had shifted on funding for social issues. Unfortunately, the data did not support my hopes. It was a punch to the gut. Our state is turning purple, and our members need to understand GAC [gender-affirming care].”[82]
The HCMS memo took TMA to task for the unsubstantiated claims made in the amicus brief[83] that TMA submitted in the case of Abbott et al. v. Doe in 2022, in support of plaintiffs challenging the governor’s directive declaring gender-affirming-care abuse under Texas law.[84] Notably, the brief claims that gender-affirming care is “medically necessary” and describes puberty blockers as “reversible.”[85]
2023: Evolution of TMA’s Gender Policies and Committee Recommendation to Ban Conversion Therapy
In 2023, TMA’s Committee on Child and Adolescent Health issued a report in favor of the resolution Banning Conversion Therapy in the State of Texas, which had been referred to the committee for evaluation in 2022.[86] The report defined “conversion” as any practice that does not “affirm” a minor’s self-defined “gender identity.”
In a 2023 TMA session, Ready, a family medicine physician who represents TMA’s Lone Star Caucus, began a process of trying to reform TMA’s gender policies from within HOD. He proposed a resolution, Gender-Affirming Care as a Monotherapy, which took aim at TMA’s policy Sexual Orientation Change Efforts and Gender-Affirmation Therapies for Minors.[87] He argued that the policy misleadingly conflates sexual orientation and gender identity and implies that “affirmation” is the only appropriate treatment for a person who declares a cross-sex identity.
The 2023 Reference Committee on Science and Public Health did not recommend Ready’s policy for adoption. Instead, they sided with the Committee on Child and Adolescent Health, recommending the adoption of the resolution Banning Conversion Therapy in the State of Texas. The Reference Committee did, however, recommend that the language on “gender identity” be removed from the “conversion therapy” component of Sexual Orientation Change Efforts and Gender-Affirmation Therapies for Minors. Ready also proposed a motion for HOD to vote on the two provisions separately, recognizing that the umbrella policy really addressed two distinct issues: sexual-orientation change efforts; and gender-affirming care.[88] As a result, one vote would address Banning Conversion Therapy in the State of Texas, while the other would address new language on “affirming-care, essentially splitting Sexual Orientation Change Efforts and Gender-Affirmation Therapies for Minors into two policies. This would also be the first time TMA acknowledged that earlier iterations of the policy involved meaningfully distinct issues.
HOD members ultimately voted for the revised version of Sexual Orientation Change Efforts and Gender-Affirmation Therapies for Minors, which defined conversion therapy only in relation to “sexual orientation.”[89] However, the older policy, which includes language on “gender identity” (55.058), was never deleted from TMA’s policy compendium, where it remains to this day.[90]
Another TMA member, Thomas Weiner, proposed an amendment to label medical transition inappropriate for minors,[91] which was in contrast to the Reference Committee’s suggested language on gender-affirming care. Weiner argued that there was no standard of care or reliable evidence base for pediatric gender medicine. LGBTQ Section members Celia Neavel and Brett Cooper testified against the amendment, asserting that such care is evidence-based and backed by all major medical associations, which recognize medical transition as “clear best practices.”[92] The amendment was defeated in an oral voting, and HOD ultimately accepted the language proposed by the Reference Committee. Members whom we spoke with speculated that the public oral vote caused many members to self-censor.
TMA’s new policy (260.139) on gender-affirming care asserts: “TMA supports physician efforts to provide medically appropriate gender-affirming care and therapies relating to gender identity and strongly opposes the criminalization of these practices;”[93] and “TMA supports the practice of evidence-based, patient-centered, gender-affirming care and will aggressively oppose the use of potentially harmful, unproven therapies for children.”[94]
As Ready’s resolution points out, the policy does not limit the use of gender-affirming care to cases of diagnosed gender dysphoria. Instead, it implies that the only eligibility criteria is the assertion of a cross-sex identity, with no need for proper assessment and diagnosis.
This seems intentional. In his testimony on the policy, John Carlo said that “my experience clinically is that there are many people that seek gender-affirming care that do not have the diagnosis of gender dysphoria.”[95] He declared no conflicts of interest.
I spoke with a member of the 2023 Reference Committee on Science and Public Health, which recommended the affirming-care resolution. This member, who had joined the LGBTQ Section in 2021, was removed from a “Group Me” chat for section members in 2023. In an email to the member, Brett Cooper explained that the chat was a “safe space” and thus could not include the member, who had publicly supported SB14, a law specifying age minimums for medical transition in Texas.[96]
The member commented that three of the six members of the 2023 Reference Committee were activists. Another member privately disclosed that they decided not to voice real concerns about the affirming-care resolution that year, out of fear. The former member also alleges that before the 2023 Reference Committee even met to discuss its position on the pro-affirming-care policy, two staffers working for the committee, Karen Batory and Christina Ly, had already drafted an interim report recommending it for adoption by the House.
The Reference Committee reportedly decided to adopt the gender-affirming-care policy as is, without submitting it for additional study, because it accepted at face value evidence supplied by Aekta Malhotra, a psychiatrist who would cohost TMA’s CME on Transgender Healthcare in 2024[97] and later serve on the 2025 Reference Committee on Science and Public Health.
That evidence consisted of a PowerPoint presentation that featured a “genderbread person”[98] and referenced the World Professional Association of Transgender Health’s (WPATH) SOC-8 guidelines. Notably, those guidelines have been deemed unsuitable for use in routine clinical practice by the U.K. Cass report and now the U.S. Department of Health and Human Services report on pediatric gender dysphoria.[99] Moreover, materials that came out of discovery in an Alabama case, Boe v. Marshall, revealed that WPATH’s guidelines were heavily influenced by politics and that the organization had suppressed systematic reviews that it commissioned after it found “low certainty” evidence for affirming care.[100]
On several occasions, the anonymous TMA member who served on the 2023 Reference Committee voiced concerns regarding the makeup of TMA sections and committees to Brad Holland, then speaker of TMA’s HOD and now TMA’s president-elect.[101] But the board took no effort to address those concerns.
2024: Adoption of TMA’s Gender Policy, Suppression of Debate, and Pushback from the Board of Trustees
After the failure of his 2023 resolution, Michael Ready remained persistent. In 2024, he proposed a new resolution to address the flaws in TMA’s new gender-affirming-care policy.[102]
Like his previous resolution, Ready’s 2024 resolution points out that TMA’s stance on pediatric gender medicine is inherently ideological and supports “gender affirmation” rather than “evidence-based” treatment for “gender dysphoria.” Ready noted that it is highly unusual for there to be only one available treatment for a medical condition. He also pointed out the importance of changing the policy, given that the American Academy of Pediatrics was currently being sued by a detransitioner for its own gender medicine policy.[103]
The 2024 Reference Committee once again recommended not to adopt Ready’s resolution, citing “majority testimony against the resolution.”[104] The committee did acknowledge that “the science continues to evolve” but claimed that “the existing policy allows for ongoing reassessment of the research.”[105] But as Ready’s resolution points out, the nuances acknowledged by the committee in its report are not reflected in the written policy, which states that gender-affirming care is evidence-based and that TMA unambiguously supports it.[106]
Around the same time, the board began pursuing organizational policies designed to stifle dissent and prevent open debate.
In 2023, the board recommended a new resolution—based on findings by the JEDI task force—establishing “Six Principles of Professional Decorum for TMA Organizational Events.”[107] One principle encourages members to report viewpoints that they deem “inappropriate” or “discriminatory.”[108] In response, TMA’s Lone Star Caucus proposed an open discourse resolution[109] modeled on the University of Chicago’s widely praised free-speech policies. The resolution was rejected, leading Ready to pen an op-ed in the Dallas Morning News exposing the climate of chilled speech at TMA and the organization’s prioritization of ideology over evidence-based medicine.[110]
In 2023, the LGBTQ and Women’s Sections introduced a resolution[111] that would have forced the Council on Legislation to establish interim policy and advocacy positions consistent with existing TMA policy. Advocates complained that TMA’s written testimony on SB14—Texas’s ban on open sex-rejecting procedures for minors—was too “neutral” a testimony and that it diverged considerably from public and organizational statements on affirming care.[112] The resolution ultimately passed, although it was softened in its final version.
2025: TMA Refuses to Assess its Gender Medicine Policies
The year 2025 offered hope that TMA might be open to reform. With the Trump administration taking a more openly aggressive approach to regulating pediatric gender medicine,[113] ongoing medical practice reversals abroad,[114] and HHS’s report on best practices for treating pediatric gender dysphoria,[115] it was becoming increasingly untenable for medical associations to claim that there was no real scientific debate over pediatric medical transition.
Some TMA members were hopeful that their attempts to revise TMA’s gender policies would achieve traction. Michael Ready drafted a resolution later introduced by the Fort Bend Medical Society that called on the board of trustees to assemble an ad hoc committee to review the organization’s policies on pediatric gender medicine, taking into account new evidence and European medical practice reversals.[116] Given what he perceived to be institutional capture at TMA, Ready believed that an unbiased committee would be better able to impartially review TMA’s policies.
Robust online testimony submitted by TMA members to the 2025 Reference Committee on Science and Public Health supported the resolution, with 17 TMA members testifying in support and only three testifying against.
Of note, two of the three dissenting testimonies came from members of TMA leadership: Robert Harold Emmick, Jr., who chaired the 2023 Reference Committee; and William S. Gilmer, former chair of the Council on Science and Public Health (CSPH) and current member of the Council of Constitution and Bylaws and an LGBTQ Section leader. In his testimony, Gilmer claimed: “As knowledge evolves and new studies emerge, the bottom-line conclusion is consistently a call for further study. With that, we all agree.”[117] This rings a bit hollow, since Gilmer seemed to have been aware of “Trojan horse” tactics exhibited by the sections, councils, and committees, which run contrary to open scientific discovery. The resolution was referred for review to the 2025 Reference Committee. Two of that committee’s six members had co-taught TMA’s CME on Transgender Healthcare the previous year.[118] A third, Shanna Combs, was a long-standing member of the LGBTQ Section.
In its decision, the 2025 Reference Committee disproportionately weighed the testimony of “subject-matter experts” over the testimony of concerned TMA members. The committee concluded that TMA policy on gender-affirming care “is sufficiently broad and adequately accounts for evolving evidence.”[119] The committee relied on an argument, made by the opponents of the resolution, that “the formation of an ad hoc committee to study one policy diverges from established TMA policymaking procedures and would be redundant to existing council and committee bodies with subject matter expertise.”
Brad Holland, then acting speaker of HOD, reportedly told a proponent of the ad hoc committee that “this is not the year for your issue.” As speaker, Holland would have been responsible for choosing the 2025 Reference Committee members tasked with evaluating the resolution.
During debate over the resolution, Ready pointed out that “only one side in the Reference Committee has presented scientific evidence in commentary, and that wasn’t the affirmation-only side. Is that a coincidence? I’m just asking to present evidence in front of an unbiased group.”[120]
But only minutes after the debate on the proposal began, it ended abruptly. As TMA members in support of the proposal were waiting to testify, an opponent moved to close debate via an unusual procedural mechanism, claiming that both sides had already been heard. Acting speaker Holland seconded this motion and, despite confusion in the House, moved on to a formal vote on the resolution. Members waiting to speak had their microphones cut. A few minutes later, Holland announced that the resolution had failed.[121]
Takeaways
- TMA’s embrace of activist positions on gender medicine is at odds with the principles of evidence-based medicine, the stated issue priorities of members, and TMA’s stated mission of serving the people of Texas and curing and preventing disease. The presence of John Carlo and Brett Cooper on TMA’s board of trustees at different points in time raises serious questions about the influence of activists on its policymaking process.
- Institutional capture arises when a small group of like-minded activists are empowered to shape policy while members with opposing views are marginalized and silenced. The need for specialized committees within large, complex organizations provides opportunity for broader institutional capture through committee capture. In this sense, the pathologies at TMA are not unlike those found in other large organizations such as Congress. The solution lies in fostering open discourse, which serves as the cornerstone of scientific debate and discovery. Equally important is the strict observance of sound governance practices.
- TMA’s LGBTQ Health Section began as an affiliation group for the purpose of supporting LGBTQ members of TMA; but through mission creep, it became the trusted source of expertise on gender medicine within TMA. The LGBTQ Health Section’s members were elected and supported for their commitment to the gender-affirming worldview.
About the Author
Joe Figliolia is a policy analyst at the Manhattan Institute. His work explores the nuances of the research literature on gender dysphoria and gender affirming care as a treatment modality, and how the state of our knowledge in this area, or the lack thereof, should inform policy decisions. Figliolia’s analysis supports MI fellow Leor Sapir, and his research and commentary on all aspects—educational, institutional, legal, scientific, philosophical—of the debate surrounding pediatric gender medicine.
Prior to joining the Manhattan Institute, Figliolia worked as a research coordinator for the MRI program at the New York State Psychiatric Institute, and as a graduate teaching assistant in Clinical Psychology at New York University. His academic interests include clinical psychology, social theory, the philosophy of psychology, and the history of ideas.
Figliolia studied psychology and English at SUNY Geneseo, where he graduated summa cum laude. He received an MA from NYU’s Center for Experimental Humanities, where his coursework focused on the philosophy of psychology.
Endnotes
Photo: A-Digit / DigitalVision Vectors via Getty Images
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).