Reining in Medicaid Managed Care

Photo: JGI/Tom Grill/Tetra images via Getty Images
Executive Summary
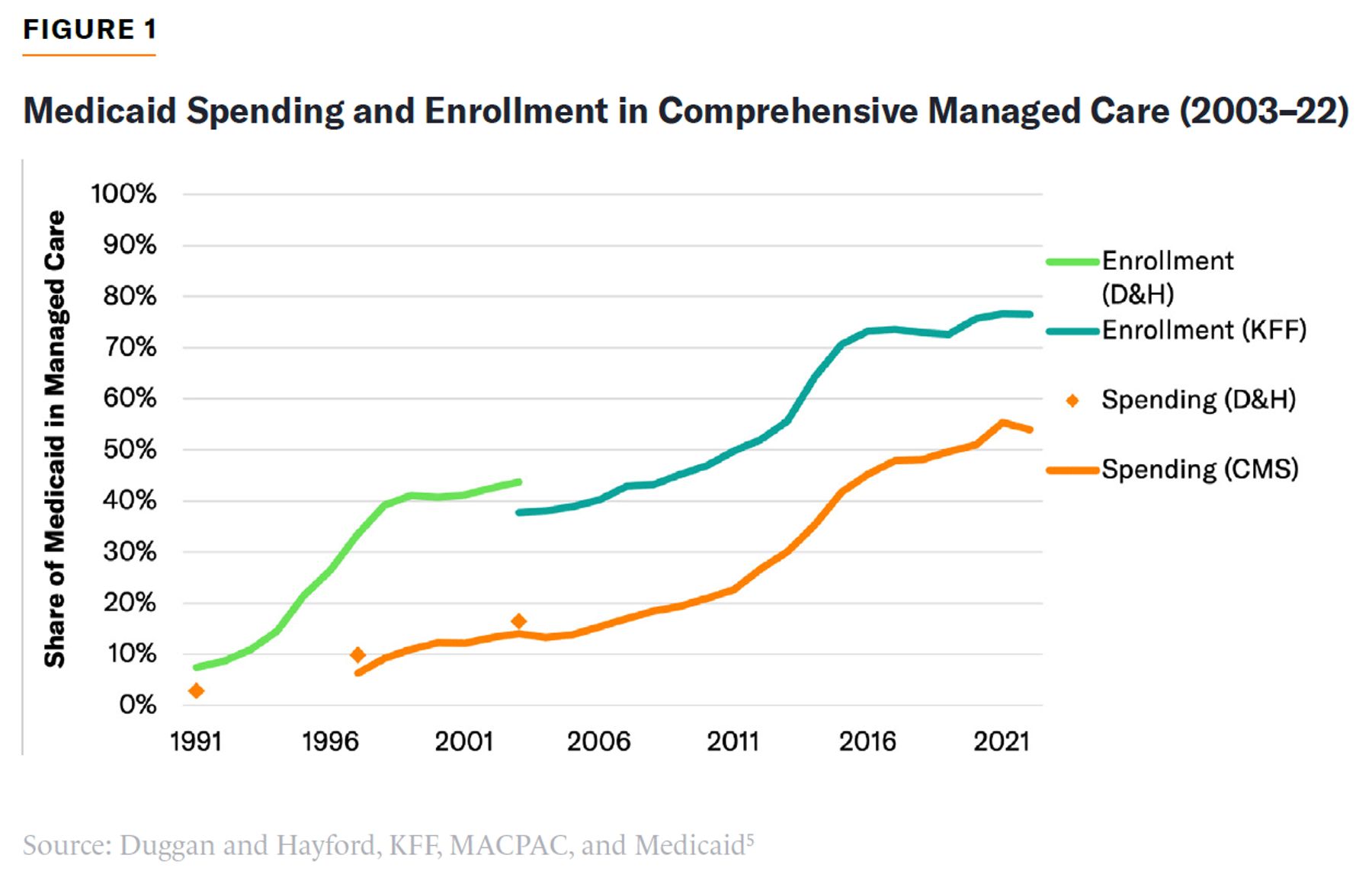
When Medicaid, the U.S. program that purchases health care for the poorest Americans, originally went into effect, states paid directly for health-care services provided to beneficiaries. But in recent decades, states increasingly subcontract procurement to private insurers known as managed care organizations (MCOs). From 1992 to 2022, the proportion of Medicaid beneficiaries enrolled in MCOs increased from 9% to 77%. This health-care delivery system of state Medicaid agencies contracting with MCOs is called Medicaid managed care (MMC).
Private insurers design benefits, raise funds, manage risk, and develop networks of providers to treat their policyholders. But in MMC, the government dictates the bulk of benefits, provides all of the revenue, carries most of the risk, and largely determines the terms of payment to medical providers.
States argue that their employment of MCOs reduces costs and improves benefits. However, payments to these private insurers are usually not set through competitive bidding; the nature of plan expenditures cannot easily be compared from state to state; and there is little evidence of savings being passed on to taxpayers. In fact, the lack of transparency has encouraged states to increasingly use MCOs to bypass traditional restrictions on the amount and purposes for which they can claim federal Medicaid matching funding.
Federal policymakers have exempted MMC from many regulatory constraints on payments for Medicaid services under the assumption that it is inherently more cost-effective. This is a mistake. Payments made to Medicaid MCOs should be subject to stricter federal controls and their activities subject to much greater transparency. This will ensure that Medicaid’s structure gives taxpayers the best value for money.
What Is Medicaid Managed Care?
Medicaid is a system of federal matching funds for states to provide comprehensive health-care benefits to low-income residents. Initially, states paid health-care providers directly to treat Medicaid beneficiaries, but over recent decades they have increasingly used private insurers known as MCOs to purchase services.
The federal government generally provides between $1 and $3 to states for every $1 that states spend on health-care benefits for most Medicaid beneficiaries, with higher-income states entitled to a higher matching rate. States may also claim $9 in federal funding for every $1 that they spend on health-care services for beneficiaries made eligible by the 2010 Affordable Care Act.
State Medicaid programs must provide a basic set of health-care and long-term care benefits to a core group of beneficiaries. But they may also claim federal matching funding to provide additional benefits to those beneficiaries or to expand Medicaid eligibility to a broader set of residents.[1]
There is no upper limit on the total federal matching funds that each state may claim for its own Medicaid expenditures. But the ability of states to claim federal funding is supposed to be limited to covered health-care and long-term care services, beneficiaries who are eligible for Medicaid, and payment amounts sufficient to enlist enough health-care providers to provide these services.
After Medicaid’s establishment in 1965, MMC was gradually expanded through waivers. The first managed care pilot was developed in 1968 in California, and managed care was implemented on a statewide basis from 1971.[2] Congress found that MCOs took advantage of this system to provide inadequate networks and engage in profiteering. In 1976, lawmakers sought to ensure quality care by limiting MCO participation to insurance plans that had more privately funded enrollees than Medicaid beneficiaries.[3] This requirement was gradually loosened before the Balanced Budget Act of 1997 formally permitted states to contract with Medicaid-only MCOs under specific regulations that ensured an adequate provider network and quality assurance.[4]
With broad support from policymakers at state and federal levels, the proportion of Medicaid spending distributed through MMC greatly expanded over recent decades. In 2022, it accounted for 77% of Medicaid enrollees and 54% of the program’s spending (Figure 1).
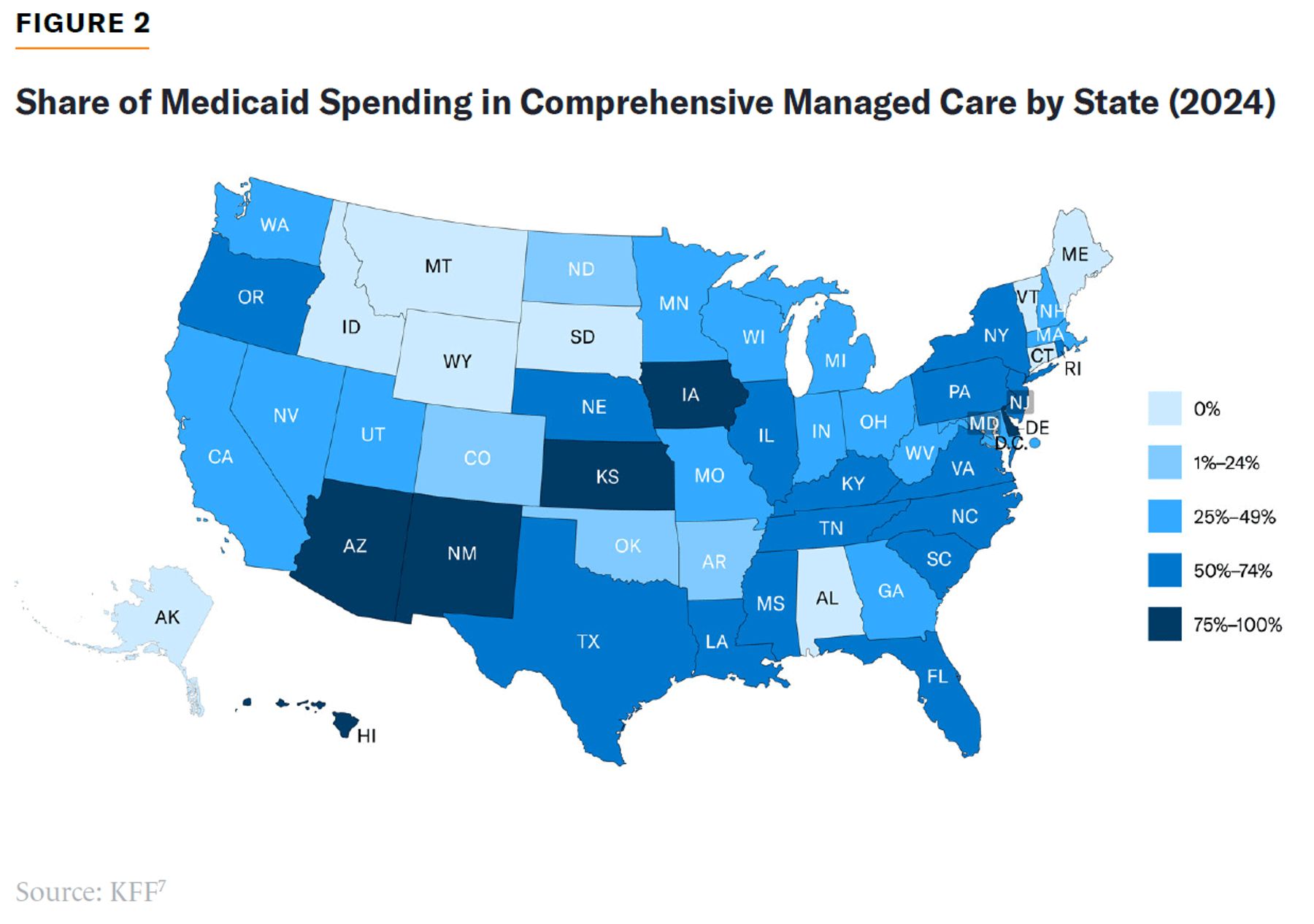
Comprehensive MMC is currently employed to varying degrees by 41 states and the District of Columbia.[6] In 2024, the proportion of Medicaid spending distributed through MMC in these states ranged from 3% in Colorado to 91% in Iowa (Figure 2).
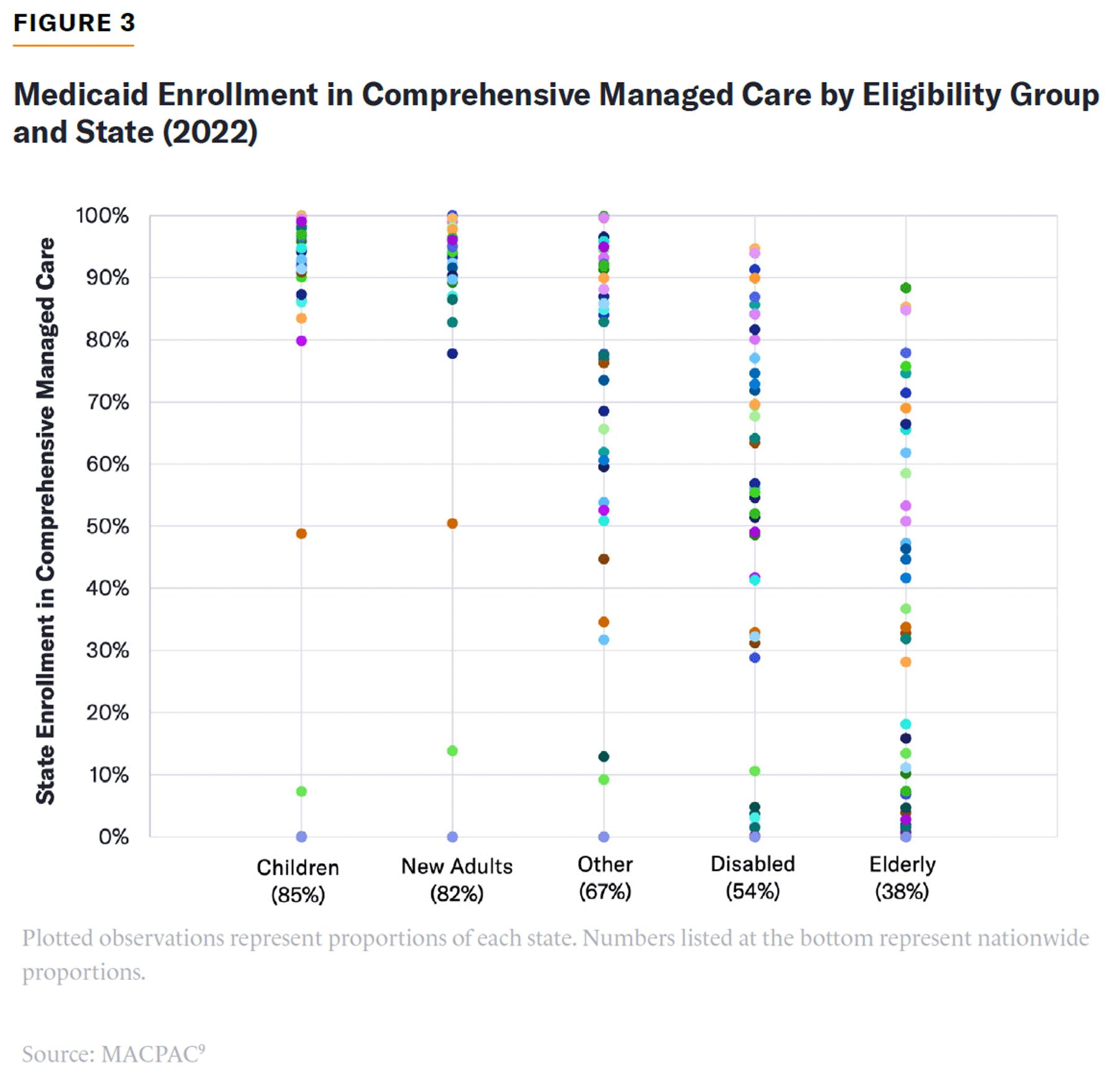
Most states use MMC to deliver Medicaid benefits to children and able-bodied adults, but many still rely on direct payments to finance services for disabled and elderly beneficiaries whose medical needs are more complex (Figure 3). Behavioral health services, substance abuse treatment, and dental care are also typically carved out of MMC contracts. In 2021, only 24 states paid for long-term care though managed care.[8] Until the 2010 Affordable Care Act allowed MCOs to claim Medicaid’s mandatory discounts on prescription drugs, most states also carved drugs out of managed care.
States may allow Medicaid beneficiaries to opt for managed care plans or may require them to do so. If states require beneficiaries to enroll in managed care, they must provide a choice of at least two plans. Beneficiaries who do not choose plans may be auto-assigned to an MCO. Nationwide, 45% of beneficiaries are in plans to which they were assigned by states.[10]
MCOs must cover all mandatory Medicaid benefits and optional benefits established by states. That means they must generally provide access to hospital and physician services without charging beneficiaries premiums or out-of-pocket costs. MCOs are subject to network adequacy requirements for primary care, specialist physicians, hospitals, pharmacists, behavioral health providers, and pediatric dentists. They must also report physician fees, service utilization, quality-of-care metrics, and denials of payment due to prior authorization.[11] States must assure the solvency of MCOs and ensure that plans spend at least 85% of their revenues on health-care services.[12]
States typically contract with MCOs for three- to five-year periods, with contracts subject to approval by the Centers for Medicare & Medicaid Services (CMS). States have wide discretion over the content of contracts beyond the minimum federal requirements.[13]
State Medicaid programs generally pay MCOs up-front monthly fees for each beneficiary enrolled.[14] Federal law requires these payments to be “actuarially sound”—in other words, “projected to provide for all reasonable, appropriate, and attainable costs.” That means they must cover the price and volume of services consumed by Medicaid beneficiaries. As a result, state payments to MCOs are typically indexed for the expected increase in medical prices.
States can set different rates for subcategories of enrollees (such as the disabled or children) or risk-adjust payments according to age and health status. These risk adjustments may be based on beneficiaries’ medical diagnoses or their use of medical services. States may also choose to compensate MCOs for certain costly patients (such as those suffering from AIDS) on a fee-for-service basis or to provide add-on “kick payments” for unanticipated costs (such as childbirth). States may provide additional bonus payments to plans for compliance with target metrics, such as the quality of medical care or reductions in racial health disparities.[15] They also often provide additional ad hoc payments to ensure the solvency of plans, if actual costs exceed earlier official projections.
MCOs have some freedom over the procurement of medical care. For example, MMC payments to hospitals are exempt from “upper payment limits” on Medicaid hospital fees, which would otherwise limit the federal matching funds for states. In 2016, CMS formally authorized “state-directed payments” to allow states to specify terms of payment from MCOs to hospitals at levels greatly exceeding those which Medicare would pay. States may also require MCOs to pay for nonmedical goods “in lieu of services,” which would not otherwise be eligible for federal matching funds.
The Debate Over Medicaid Managed Care
MMC was intended to bring the advantages of private administration and managed care to Medicaid. Rather than funding whatever services are delivered to Medicaid beneficiaries, paying insurers up front to cover enrollees can incentivize them to procure the most cost-effective treatment. In private insurance, managed care has cut the cost of health care by reducing the price and volume of medical services employed.[16] In Medicare, private managed care plans have improved medical outcomes by providing additional preventative care services, which avoid costly hospitalizations.[17]
But private management fits awkwardly within Medicaid. As the benefit is financed almost exclusively by public funds, plans have no incentive to compete for enrollees by reducing premiums.[18] Nor can they charge higher premiums in return for providing better-quality coverage. Since they must accept all beneficiaries in return for public funds (with imperfect adjustments for medical needs), plans have a strong incentive to skimp on costly medical services that are most attractive to seriously ill beneficiaries. As a result, Medicaid benefits tend to be highly standardized by law, which leaves little opportunity for desirable innovation by insurers.
Care Procurement
Private insurers have little scope to reduce the prices that Medicaid pays for medical services. Whereas managed care uses narrow networks to reduce the fees private insurers pay for medical care, Medicaid already typically pays low rates for health care due to mandatory discounts and price controls. When states pay for services directly, Medicaid networks are already narrow.
Administration by MCOs does little to eliminate the desire of state legislatures to micromanage Medicaid programs and support favored providers. States worry that MCOs have an incentive to exclude good-quality providers to deter sicker beneficiaries from enrolling with them.[19] Under MMC, state law often mandates that covered networks of providers include relatively costly hospitals, such as rural hospitals or academic medical centers. States often do not want MCOs to squeeze the revenues of safety-net providers; therefore, in 2016, CMS allowed states to specify the precise fees and add-on payments that MCOs must make to facilities.[20]
MMC can be used to broaden or narrow Medicaid’s provider networks. It creates a firmer legal obligation to assure an adequate network and is often viewed as a way to tie the program’s networks to higher standards employed by private insurance. But network adequacy regulations vary greatly, and enforcement is often loose.[21] Many providers that are nominally part of Medicaid networks are, in practice, often unwilling to accept new Medicaid patients.[22] A quarter of primary care physicians provide 86% of primary care to MMC patients.[23] It may be easier for states to ensure satisfactory access to care by paying for it directly rather than through MCOs.
Federal law already entitles state Medicaid programs to the lowest prices on drugs while prohibiting the use of formularies to negotiate further discounts.[24] MCOs may still employ prior authorization and modest co-pays to steer beneficiaries to use cheaper branded and generic drugs, but the savings to be obtained are much smaller than those available to other forms of insurance.
Utilization Controls
MCOs have the ability and incentive to review the necessity of costly medical services before approving their use. Such prior authorization generates substantial savings in Medicare Advantage and is potentially particularly valuable in Medicaid, where the utilization of health-care services is typically unconstrained by patient cost-sharing.
Although some states already employed forms of prior authorization and gatekeeping of access to specialty care before adopting managed care, these generally require a larger amount of administrative staff than states are willing to hire directly.[25] MCOs employ many clinicians who can assess whether proposed treatments are medically necessary and cost-effective, as well as pharmacists who are able to handle medication management. MMC can therefore replace cruder methods of rationing (such as price controls on physician services or quantity limits on drugs) with more clinically nuanced assessments of the value of services to patients in particular situations.
But Medicaid MCOs may be overzealous in denials of access to care. Unlike the Medicare Appeals Council under Medicare Advantage, MMC has no automatic independent review of denials and rarely much regulatory oversight of the process.[26] MCOs denied 13% of requests for prior authorization in Medicaid, compared with 6% in Medicare Advantage.[27]
Whereas prior authorization for privately funded insurance can admit multiple thresholds of medical necessity, reflecting how private payers vary in their willingness to pay for different levels of intensity of care, a publicly financed safety-net program needs only one.
Benefit Innovation
In theory, MCOs have an incentive to provide additional preventive care services to keep patients healthy. This is not just because they stand to save money by avoiding costly hospitalizations, but also because beneficiaries will prefer plans that offer a better quality of care, while states can reward plans with the highest-quality ratings.
But it is hard for states to identify, monitor, and fully specify quality of care in contracts with MCOs. Quality metrics may be easy to game, may be costly to administer, and may do more to reward plans for enrolling healthier patients than for making sicker patients healthier. There is little evidence to support some policymakers’ claims that requiring medical providers to bear the costs associated with adverse medical outcomes improves the quality of care. But the additional spending required to entice providers to participate in risk-bearing payment models does seems to increase costs.[28]
Potential savings from preventative services, beyond those covered by conventional health-care benefits, are often exaggerated. This is particularly true for expenditures on services to address “social determinants of health.” Although poor housing is correlated with ill health, public expenditure on housing assistance typically fails to generate substantial savings in health-care expenses.[29] Because the typical Medicaid beneficiary is enrolled for less than 10 months, plans are unlikely to provide many supplemental services under the expectation that they will pay for themselves.[30]
In fact, the effective delivery of preventative care services, such as vaccinations, may be easier to ensure if states pay for them directly and transparently on a fee-for-service basis. This is also true for care coordination services, which are often most necessary for patients with idiosyncratic medical and behavioral problems, for whom it may be difficult to specify service requirements in MCO contracts. In most cases, MCOs will just subcontract case management services anyway.
States have increasingly made MCOs responsible for long-term care, under the theory that it would lead them to provide home-based services for beneficiaries to live independently at a fraction of the cost of 24-hour nursing facility care, which can reach $100,000 per year.[31] Yet as it is easier for MCOs to identify additional beneficiaries who are eligible for long-term care funding than it is for MCOs to return those who are already in nursing homes back to independent living, incorporating long-term care into MMC has tended to push the program’s spending up rather than down.[32]
Furthermore, because long-term care recipients are often frail and socially isolated and suffer from serious cognitive impairment, there is a high risk of inadequate or substandard care. That may be harder for states to police if information about payment and utilization of long-term care services is intermediated by MCOs. A Government Accountability Office audit found that CMS failed to detect real problems in quality and access to managed long-term care benefits and lacked the information or strategy needed for effective oversight.[33] The paucity of public data on MCOs’ internal operations has generally precluded assessments of the efficacy of managed long-term care programs.[34]
Administrative Overhead
In 2016, states that employed MMC to purchase health-care services had only slightly lower direct administrative costs (4.9%) than those that paid for care directly (5.8%).[35] Where MCOs are responsible for purchasing care, states must still ensure that insurers are not themselves claiming excessive public funding. Furthermore, every state still operates a residual fee-for-service program for populations carved out of managed care and so must also maintain the infrastructure needed to directly pay health-care providers.
MCOs also impose administrative expenses on top of those borne by states. They must negotiate contracts with states and medical providers alike, advertise plans to beneficiaries, comply with extensive regulations, finance adequate capital reserves, and generate profits for investors. The larger the number of MCOs involved in a state’s Medicaid program, the greater the costs associated with contracting, monitoring, and mitigating adverse selection.
To the extent that MCOs attempt to manage the care that is delivered, this also increases administrative expenses. Federal rules penalize MCOs with administrative costs exceeding 15% of their expenditures, but they can easily manipulate this metric by recategorizing expenses or passing them downstream to medical providers.
Paying MCOs
Even where MCOs generate substantial savings in the procurement of medical care, these are typically not passed on to taxpayers. In 2017, 32 states established payments for MCOs by administrative fiat, while only 6 states set rates through formal competitive bidding.[36] States are wary of pure competitive bidding because this would leave the program controlled by a single MCO, which would become hard to discipline. Furthermore, merely contracting with the lowest bidder would risk placing all enrollees with a single MCO that has most underestimated the cost of coverage and cannot cover the associated expenses.
However, the absence of competitive bidding means that plans have little incentive to reduce the cost of delivering the intended Medicaid benefit. This is further undermined by actuarial soundness requirements or financial standards that ensure the plan has enough resources to meet its future benefit obligations reliably. These requirements dictate that states pay MCOs at least 100% of expected health-care and administrative costs—an arrangement that encourages MCOs to expand expenditures.[37] These requirements may lock states into higher Medicaid expenditures for the three- to five-year duration of MCO contracts—prohibiting them from trimming excessively expensive programs.[38] In fact, actuarial soundness requirements encourage MCOs to pay providers fee-for-service because that increases the number of recorded encounters on which payment adjustments to plans are based. This process negates the intended cost-saving incentives at the heart of managed care.[39]
States struggle to avoid overpaying MCOs. Insurers have better data about costs, utilization, and market conditions than understaffed state Medicaid agencies. State officials are less experienced, are less well paid, and have less skin in the game than MCOs, with whom they may have an eye to future employment when negotiating rates.[40] States rely heavily on the same few actuarial firms employed by insurers and thus have little ability to push back on assumption embedded in data. The more MCOs states contract with, the lower the average quality and value for money they must be willing to accept.
The historical cost of a fee-for-service benefit initially provides a benchmark against which the appropriateness of payments to MCOs can be assessed. But over time, increases in health-care costs, the development of medical technologies, and changes to the package of covered benefits mean that the adequacy of rates proposed for MCOs can only be compared with one another—and each MCO has an interest in justifying higher rates.
The process of contracting with MCOs is also troubled.[41] States have great difficulty enforcing penalties, ensuring compliance with data-reporting requirements, and adjusting overpayments to plans. Initial terms of payment are rarely implemented exactly as originally agreed, with MCOs constantly seeking ex post adjustments to account for changing circumstances. Minor changes to contracts can be subject to years of litigation, which can be profitable for MCOs even if they lose in court by extending the duration of payment arrangements. States cannot easily wield the threat of not renewing MCO contracts due to the threat of litigation, the dependence of program stakeholders on existing benefit arrangements, the political influence of insurers, and the desire of states to maintain multiple participating MCOs operating at sufficient scale.
Flexibility
MMC appeals to many politicians because it appears to allow them to set broad objectives and let MCOs take care of many painful details of implementation. This may allow difficult trade-offs to be depoliticized and made on their economic merits. But fixed amounts paid to MCOs in advance for each patient they cover (capitated payments) do not preclude interest groups from pressing legislatures to mandate terms and fees for specific services. Indeed, MCOs may make this easier by allowing provider interest groups to frame the struggle as between themselves and unpopular profit-making insurers rather than the public purse.
MMC does little to make Medicaid costs more predictable for states. The unpredictability of Medicaid spending comes largely from fluctuations in enrollment associated with the business cycle and the increase of medical supply costs. States, rather than MCOs, continue to bear the risk of additional costs resulting from these factors. In fact, multiyear MCO contracts make it harder for states to respond to unanticipated cost increases by adjusting payments to providers, altering eligibility, permitting waiting lists, or trimming the package of covered benefits.
In practice, MMC fragments insurance pools into smaller subpopulations, and MCOs insist on being paid extra to enroll beneficiaries with more uncertain medical costs. MMC is typically limited to able-bodied beneficiary cohorts whose medical needs are the most straightforward, while those with special needs are usually carved out of managed care.[42] After adjustment for the number of enrollees, compensation for changes in medical prices, carve-outs of complex services, risk-adjustment payments, outlier payments, risk corridor subsidies, and so on, MCOs bear very little risk—but are often paid extra as if they do.
Program Integrity
Prior authorization allows MCOs to prevent improper reimbursement claims by medical providers. But plans may lack the incentive to do so; improper claims push up the payments that states are required to provide to MCOs by actuarial soundness requirements, while also helping them to satisfy the regulatory requirement that they spend 85% of their revenues on payments for medical services.
MMC creates an additional risk that MCOs will claim substantial fixed payments for enrollees who receive no services from the program. In 2022, Medicaid paid for 26 million more enrollees than the number of people who survey data suggested were enrolled in the program.[43] CMS estimated that in 2024, Medicaid plans were likely paid to cover 3 million Americans who were also covered by Exchange plans or Medicaid in another state.[44] A federal audit of California’s Medicaid program discovered that more than half of Medicaid plan enrollees surveyed were either ineligible for benefits or enrolled without appropriate proof of eligibility.[45]
Even when MMC enrollees are legitimate, it is hard to stop MCOs from claiming overpayments for them. In Medicare Advantage, federal analysts estimate that payments to insurers have been increased by 12% as a result of their attempts to exaggerate beneficiaries’ health-care needs.[46] No similar analysis has been undertaken for MMC, but the problem is likely to be even more substantial, because Medicaid covers services such as long-term care for which needs are more susceptible to exaggeration.
Furthermore, states have fewer resources with which to police overpayments than the federal government does when directly administering Medicare, and less incentive to do so because the majority of savings would go to a different level of government. According to a 2021 federal investigation, only 8 of 39 MMC states provided complete and accurate data for the medical service utilization on which payments to providers for the state’s largest plan were based.[47]
Accountability
When pressed, it is striking how many Medicaid officials suggest that the value of MMC is that it allows them to do things that would not be politically easy for them to do directly and transparently.
MMC makes it harder to keep track of what the program is paying for. Former Connecticut House Speaker Chris Donovan lamented of MCOs,“Obtaining information about how they were performing with the taxpayers’ money was a major fight, involving litigation under the Freedom of Information Act and other frustrating efforts at holding them accountable.”[48]
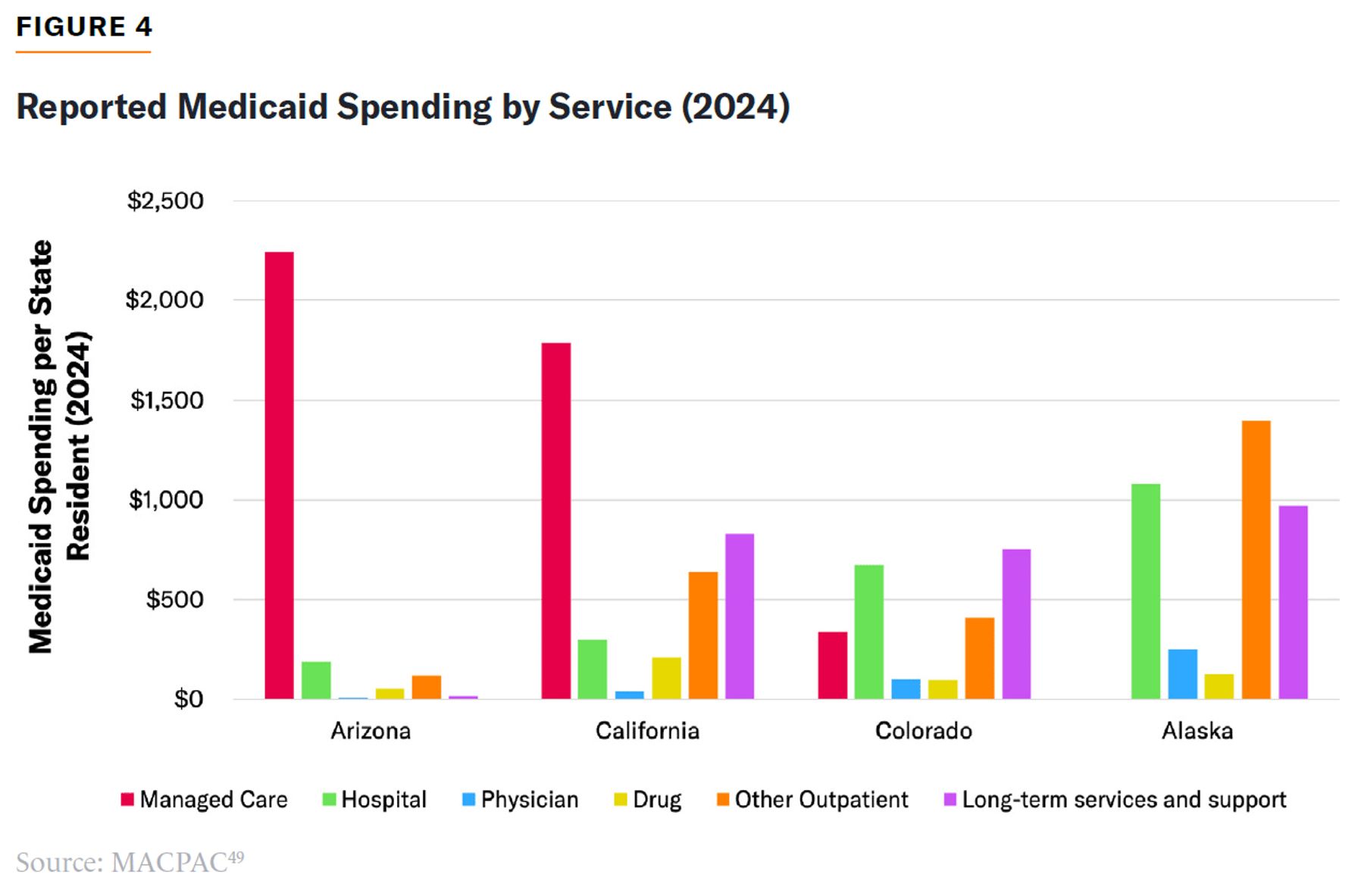
This difficulty of getting critical information is greatly multiplied for anyone not directly involved in contracting with MCOs. States lump together expenditures for all different services as “managed care” when reporting their annual expenditures to CMS (for example, Figure 4). That makes it impossible to compare the Medicaid services that different states are purchasing and the value that taxpayers are obtaining in return for federal funding.
Fiscal Shenanigans
Because there is no limit on the overall amount of Medicaid matching funds that states can claim from the federal government, each state has an incentive to artificially inflate their program’s recorded expenditure.
Perhaps the most important consequence of MMC now is its impact on state–federal fiscal relations.[50] States traditionally designed MMC responsibilities so as not to impede existing schemes to draw Medicaid “supplemental payments” from the federal government.[51] In recent years, states have used MCOs to inflate Medicaid matching funds and draw supplemental windfalls from federal taxpayers on an unprecedented scale.
MMC allows states to claim more federal aid for the same state contribution to Medicaid. Whereas the federal government provides only $1 in funding for every $1 that states spend on Medicaid administrative expenses, states can claim up to $9 for every $1 that is spent on administering claims by MCOs because those expenditures are matched as if they were medical care.[52]
States have also used taxes on MCOs to fleece federal taxpayers. California obtained a $19 billion windfall in federal funding over four years by imposing a tax on MCOs in return for higher Medicaid payments to them.[53] Seven states mimicked the scheme before CMS finalized a rule to restrict permissible taxes on insurers in early 2026.[54] Under the Medicaid Voluntary Contribution and Provider-Specific Tax Amendments of 1991, states were already supposed to be prohibited from imposing targeted taxes on MCOs as a quid pro quo for higher federal Medicaid funding, but California managed to structure the arrangement to avoid restrictions. It seems likely that states will find ways to evade the new restrictions on such scams.
States have also increasingly used MCOs to claim federal Medicaid matching funds for non-health-care social service expenditures. For instance, Arizona, California, Mississippi, Nevada, Ohio, and Oregon all mandate that Medicaid MCOs contribute funds to state housing policy initiatives as a condition of their contracts.[55] Centene and UnitedHealth are reported to have made billion-dollar expenditures on “affordable housing” developments.[56] Payments to MCOs to claim matching funds for such expenditures on noncovered benefits are supposed to be capped at 5% of payments to plans, but the federal government has little capacity to monitor and enforce such limits.[57]
MCOs had been exempt from Medicaid’s traditional rules that limit states’ ability to claim federal matching funds for hospital services to no more than what Medicare would pay for the same services. States realized that this exemption allowed them to use MCOs to draw an enormous additional windfall in federal matching funds by mandating that MCOs make higher payments for health-care services, known as state-directed payments (SDPs). From their establishment in two states in 2016, SDP mandates on MCOs grew to a projected $124 billion across 39 states in 2025.[58] In this scheme, states claim federal funds to pay hospitals as much as six times Medicare rates, the bulk of which went to academic medical centers, whose own Medicare rates are often double the average for hospitals.[59] Of the state matching contribution to this increase in federal Medicaid payments to hospitals, 81% was “financed” by state taxes on health-care providers.[60]
There have since been modest attempts to rein in SDPs. In 2024, the Biden administration limited the amounts that Medicaid MCOs could claim for hospital care to 2.5 times Medicare rates.[61] The 2025 One Big Beautiful Bill Act limited new SDPs to Medicare rates and established a gradual phasedown of existing SDPs to Medicare rates.[62] It remains unclear whether these constraints will be allowed to take full effect or states will find ways around them.
CMS lacks the resources to do thorough oversight of every state’s complex MCO contracting arrangements. Whereas MCOs will vigorously challenge underpayments with litigation, overpayments face little pushback. The astonishing growth of SDPs calls into question MMC’s core budgetary guardrails. If states and MCOs claimed that pre-SDP rates were actuarially sound, then how could the much higher post-SDP rates also be actuarially sound payments for the supposedly same services?
Evidence on MMC
A substantial body of research has attempted to determine whether MMC improves or worsens the efficiency of the Medicaid programs.
Sara Rosenbaum and Maria Casoni recently suggested, “No health policy undertaking is more complex than Medicaid managed care.”[63] Medicaid eligibility, benefits, and provider payments already vary greatly across states, and procuring services indirectly through MCOs adds a further layer of complexity to arrangements. This is heightened by the reluctance of insurers to disclose the details of what they regard as proprietary provider payment arrangements.
A 2002 Urban Institute review of the development of MMC noted that its 1990s expansions were driven by a widespread faith that it would generate savings “despite very scant evidence.”[64] In 2018, a Congressional Budget Office report noted that while proponents suggest that MMC “reduces spending and improves outcomes,” studies “have not found consistent evidence to support those claims.”[65]
States’ Transition Experiences
The impact of MMC can be observed in states that have recently reformed their programs.
Kansas originally claimed that its 2013 shift to MMC would reduce costs by 10% due to the addition of care coordination and preventative services. But this did not occur. Costs remained high, and MCOs suffered losses of 20%. Payments to plans were then increased by 11% relative to their previous level, amid reports that MCO provider networks were inadequate and claims were often improperly denied.[66]
Iowa was similarly unable to obtain savings from its 2016 transition to MMC. MCOs reported losses of more than 10% in the first year, and the state was forced to establish a “risk corridor” bailout for plans.[67]
Connecticut abandoned MMC in 2011, following a state audit showing that the state had been overpaying plans by 5% to 6% and other reports suggesting that MCOs spent an inadequate share of revenues on medical services.[68] The state claims the shift back to direct payment for care reduced administrative costs from 12% to 5% and increased the number of physicians willing to treat Medicaid patients by 7%.[69]
Implications
Numerous econometric assessments of the impact of MMC have been undertaken. For a table summarizing each of these peer-reviewed publications, see the Appendix.
The studies cited in the Appendix are consistently well designed and methodologically sound, but yield limited and seemingly contradictory conclusions about the impact of MMC. Some of them find that MMC expands the quality and scope of Medicaid benefits. Other studies find reduced access to medical care. Some find that it increases the program’s level of spending; others find that it reduces it.
These disparate findings reflect the fact that the introduction of MMC is typically coupled with other changes in Medicaid benefits. MMC does not necessarily alter the level of spending that states will decide to devote to Medicaid. States can use MMC to expand benefits; they can also employ it to narrow them.
MMC is clearly capable of cutting the cost of Medicaid benefits by reducing the utilization of health-care services. But there is a consistent trade-off between cost and quality or access to care, as there is with attempts to reduce expenditure within fee-for-service Medicaid programs.
There is no robust evidence that MMC delivers a clear gain in efficiency, i.e., an improvement in the quality of medical care coupled with reduced costs to taxpayers. In fact, Medicaid MCOs have not achieved the same reductions in prices and preventable hospitalizations that MCOs did in private insurance.
The precise impact of MMC on various types of Medicaid expenditures cannot be easily identified due to the degree to which MMC impedes reporting of the program’s expenditures across service categories. That makes it difficult to determine whether changes to aggregate levels of expenditures represent improved value for taxpayers or merely a drain of resources to the profit of MCOs.
This absence of transparency and its implications for accountability are likely the most significant consequences of subcontracting the administration of Medicaid to MCOs. This is particularly true with respect to the impact of MMC on attempts by states to inappropriately inflate federal matching funds—where MMC is valued by states precisely because it makes fiscal shenanigans difficult to identify.
Recommendations
To make MMC more accountable and ensure that Medicaid expenditures are used most efficiently, Congress should:
- Close MMC loopholes from limits on Medicaid funding.
MMC allows states to claim more federal funding for the same amount of health-care services than they otherwise could. This is because MMC is exempt from restrictions on the services for which states may claim federal matching funding. MMC also loosens the caps on the amount of aid that states may claim for each health-care service. The auxiliary restrictions used to constrain funding of MCOs (such as budget neutrality requirements, medical loss ratio limits, and actuarial soundness conditions) are loose, easily manipulated, and ineffective substitutes.
States should not be allowed to claim federal funding for MMC payments to providers that exceed traditional upper payment limits; nor should they be permitted to claim additional funding for noncovered benefits provided in lieu of service. States should also be entirely prohibited from imposing taxes on any MCO that receives Medicaid funding. - Standardize MCO contract and payment terms.
MCO contracting is needlessly complex, litigious, and costly. States are poorly equipped to design, oversee, and enforce contract terms, whose idiosyncrasies also inhibit federal oversight. The absence of competitive bidding means that MCOs are typically overpaid, with payment often deliberately designed for the purpose of improperly inflating federal matching funds.
Nationally standardized MCO contracts would allow a consistent set of payment rules to be applied across the country, making clear the extent to which plans are being overpaid for various services they provide. It would also help states avoid litigation over payment obligations and provide a more consistent assurance of baseline health-care quality, while also reducing reliance on private actuaries and consultants who are often compromised by their relationships with MCOs. - Require consistent reporting of MCO expenditures.
MCOs argue that the terms by which they procure health-care services are trade secrets. But MMC is a business that exists exclusively to serve government demand. It is essential for policymakers to know what specifically they are getting in return for their money, and transparency on this point is an essential element of the product. MCOs should report expenditures by service and beneficiary in the same manner that states are required to for fee-for-service expenditures. - Allow states to outsource claims administration to CMS.
States often employ MCOs because they lack the bureaucratic capacity to directly administer claims and because they can claim federal funding at a higher matching rate for this administration to be undertaken by MCOs. That inadvertently makes it harder for the federal government to monitor the appropriateness of spending. CMS already has the bureaucratic capacity to administer Medicare and Medicaid payments, even for subpopulations of beneficiaries with the most complex medical needs, who are typically carved out of MMC.
Because CMS is involved in monitoring the adequacy of provider networks and overseeing the legitimacy of Medicaid claims administered by states, making it directly responsible for payment would eliminate a layer of needless bureaucratic cost. From a federal budgetary point of view, there is an advantage to CMS being able to directly monitor claims, so Congress should allow states to employ CMS to directly administer claims without requiring states to make any contribution to the expense.
Conclusion
Subcontracting Medicaid to private insurers with MMC was originally intended to increase innovation and improve the efficiency of the program. But Medicaid benefits are highly standardized by law, and premiums paid to plans are typically not subject to competition. Whatever efficiency gains that MCOs may generate are usually more than offset by additional expenses they incur. Furthermore, MMC reduces the accountability of Medicaid by making it harder for policymakers to identify and adjust the drivers of the program’s spending growth.
The lack of transparency by MCOs has helped states inflate the federal funding they receive beyond what they are entitled to. Federal policymakers should not assume that MMC necessarily reduces costs. In fact, they should be wary that states are often embracing it primarily for the purpose of fiscal shenanigans and should enact reforms to make Medicaid expenditures easier to track.
Appendix
Econometric Analyses of Transitions
Various econometric analyses have attempted to disentangle the effect of MMC from confounding circumstances and the skewed voluntary selection of beneficiaries into managed care. The most common method employed to identify the impact of MMC has been to use staggered county-by-county differences in the timing of the mandates for Medicaid beneficiaries to enroll in MMC.
| Study | Identification Strategy | Finding |
| Azier, Currie, and Moretti, 2007.[70] | MMC mandate phase-in, California counties 1990–2000. | Prenatal care in first trimester fell 4–8% when in MMC. More low birthweight and neonatal death. |
| Kuziemko, Meckel, and Rossin-Slater, 2017.[71] | MMC mandate phase-in, Texas counties 1993–2006. | Black mortality increased by 15% and preterm birth increased by 7%. Hispanic mor-tality reduced 22% and preterm birth reduced 7%. Suggests selection of low-risk enrollees. |
| Chorniy, Currie, and Sonchak, 2018.[72] | MMC mandate phase-in, South Carolina counties 2004–15. | Risk adjustment created incentive for provid-ers to diagnose and prescribe medications for ADHD, asthma, and other conditions with nebulous diagnoses. |
| McConnell et al., 2023.[73] | Elimination of behavioral health carve-out, Washington counties 2014–19. | No significant difference in service utiliza-tion, quality, or health outcomes. |
| Kwon et al., 2024.[74] | MMC mandate phase-in, Pennsylvania counties 2010–18. | Earlier detection of cancer; MMC reduced probability of late-stage diagnosis by 7%. |
| Bhaumik et al, 2025.[75] | Managed long-term services and supports (MLTSS) mandate phase-in, across states 2004–18. | MLTSS increased home care use 2.5 per-centage points and reduced informal care 3 percentage points. No change in nursing home use or health outcomes. |
| Lee et al., 2026.[76] | MLTSS mandate phase-in, Florida and New York counties 2012–15. | MLTSS adoption reduced utilization of primary care (2–6%), specialists (2–7%), labs (2–4%), drugs (0.5–0.8%), and outpatient emergency department (ED) (6–7%). Hospital-izations increased (0–4%). |
| Duggan and Hayford, 2013.[77] | MMC mandate phase-in, counties 1991–2003. | No significant change in Medicaid spending. |
| Layton and Politzer, 2024.[78] | MMC mandate phase-in, counties 2004–15. | MMC reduced fiscal cost 2% in year 1 but in-creased it 10% after year 4. Implies 19% cost increase, as only half became enrolled. |
| Van Parys, 2014.[79] | MMC mandate phase-in, counties 2006. | Insurer-owned MCOs reduced costs 7–12% due to reduced hospital spending. |
| Layton et al., 2019.[80] | MMC mandate phase-in for dis-abled, Texas counties 2007. | MMC eliminated quantity limits on prescrip-tion drugs and reduced inpatient spending 8%. Total spending up 12%. |
| Bögl, 2025.[81] | MMC mandate phase-in for dis-abled, California counties 2011–12. | MMC increased ED use 4% and mortality 7%, concentrated among beneficiaries with chronic conditions. |
| Lee, 2025.[82] | MMC mandate phase-in, New York counties 2004–10. | MMC quality incentives increased office visits 25%, child immunization 27%, and spillover into higher utilization by privately insured. |
| Dranove, Ody, and Starc, 2017.[83] | Carve-in of prescription drugs to MMC, states 2010–16. | MMC reduced drug spending by 22% due to steering to cheaper drugs and pharmacies. No change in overall drug volume. |
Other Econometric Analyses
As MMC mandates are often accompanied by other changes to Medicaid benefits, they may not identify the impact of MMC as distinct from other elements of reform packages. Other research approaches, such as regression discontinuity studies or the random assignment of beneficiaries, have therefore been used to identify the difference that MMC makes to existing beneficiaries.
| Study | Identification Strategy | Finding |
| Lee, 2017.[84] | Discontinuity exclusion of birth weight <1.2kg from MMC, New York 1995–2013. | MMC reduced hospital length of stay and hospital costs by 6%. No significant impact on mortality or readmissions. |
| Lee and Vabson, 2024.[85] | Discontinuity exclusion of birth weight <1.2kg from MMC, New York 2004–10. | MMC assignment increased enrollment 49 percentage points, of which 38% remains at age 4. Attrition lower among costlier beneficiaries, suggesting MMC offers better routing care. |
| Kreider et al., 2024.[86] | MCO adds top cancer hospital, New York 2005. | Enrollment increased 50% among those with cancer. MCO subsequently dropped the hospital from its network. |
| Macambira et al., 2022.[87] | Random assignment of enrollees to MMC, Louisiana 2010–16. | MMC reduced spending by 6%, 80% of which was due to generic substitution reducing drug spending by 25%. 2% less primary care; 14% more emergency room (ER) use. |
| Marton, Yelowitz, and Talbert, 2017.[88] | Auto-assignment of beneficiaries to MCOs, Kentucky 2011. | Most remained in assigned low-cost plans. Substantial adverse selection with 10 percentage points more high-cost enrollees switching out of plans. |
| Swaminathan et al., 2020.[89] | Auto-assignment of beneficiaries to MCOs, 2009–13. | Beneficiaries assigned to Medicaid-only MCOs had 20% fewer outpatient visits and 38% less specialty care, but similar ER and inpatient use by mainstream insurers. |
| Geruso, Layton, and Wallace, 2020.[90] | Random assignment to MCOs, New York 2008–12. | Assignment to lowest-spending MCO reduced spending by 33% and increased avoidable hospitalizations 15%. Driven by reduction in high- and low-value care across hospital, outpatient, and drugs. |
| Layton et al., 2024.[91] | Transition of beneficiaries to Medicare at age 65, 2008–15. | Medicare had 27% higher costs for MMC enrollees, but 12% for fee-for-service (FFS) Medicaid. Extra cost for FFS was mostly due to higher prices. Data detail was unavailable for MMC. |
| Politzer, 2025.[92] | MCO exits from counties, 2006–14. | MCO exits reduced spending by 7%. Primary care visits reduced 10%, prescription drug use reduced 16%, and hospital admissions were up 8%. |
About the Author
Chris Pope is a senior fellow at the Manhattan Institute. Previously, he was director of policy research at West Health, a nonprofit medical research organization; health-policy fellow at the U.S. House Committee on Energy and Commerce; and research manager at the American Enterprise Institute. Pope’s research focuses on health-care payment policy, and he has recently published reports on hospital-market regulation, entitlement design, and insurance-market reform. His work has appeared in, among others, the Wall Street Journal, Health Affairs, U.S. News & World Report, and Politico.
Pope holds a B.Sc. in government and economics from the London School of Economics and an M.A. and Ph.D. in political science from Washington University in St. Louis.
Endnotes
Are you interested in supporting the Manhattan Institute’s public-interest research and journalism? As a 501(c)(3) nonprofit, donations in support of MI and its scholars’ work are fully tax-deductible as provided by law (EIN #13-2912529).